MCV Campus Ginger Edwards DISCLOSURES George W Vetrovec




































 • Advance")














- Slides: 55
MCV Campus Ginger Edwards
DISCLOSURES George W. Vetrovec, MD Consulting Fees – Gilead Sciences, Merck & Co. , Inc. , Abbott Vascular Honoraria – Cordis, a Johnson & Johnson company, Eli Lilly and Company, Daiichi Sankyo, Inc. , Gilead Sciences Grants/Contracted Research – Corindus, Inc. , Cordis, a Johnson & Johnson company, Merck & Co. , Inc.
Percutaneous Coronary Intervention: Basic Techniques George W. Vetrovec, MD. VCU Pauley Heart Center MCV Campus Virginia Commonwealth University
PCI Basics • • • Radiation Safety Angiography Contrast Volume Anatomic risk assessment of procedure Pharmacology Equipment use Stent Deployment Follow-up Angiography Compliance
Radiation Safety • In PCI flouro accounts for more radiation than Cine • Never fluoro when not viewing • Multiple views • Shielding • One Step Rule
Coronary Angiography
Contrast Volume Limit!
Coronary Angiography Coronary Intervention: Optimal Coronary Angiography Goal is to adequately opacify coronary artery without streaming • Properly positioned catheter • Sufficiently large catheter lumen for necessary and available contrast injection (including the inside “equipment”) • Always insure “reflux” (defining ostium)
Optimal Coronary Injection Pattern Dehmer & Popma: Cathsap III
Coronary Angiography for PCI • Get a Clear View of vessel and lesion anatomy including side branches. • Better yet, get two high quality orthogonal views. • If the wire is not going properly in your “best view” look in a second view.
Proximal Ramus Stenosis
Coronary Angiography Lesion Classification: Coronary Angiographic Outcomes Predictors Based on AHA/ACC Grading System Type A Discrete Concentric Readily accessible Smooth Contour Little or no calcification Non ostial No major side branch involved Absence of thrombus
Coronary Angiography Lesion Classification: Coronary Angiographic Outcomes Predictors Based on AHA/ACC Grading System Type B Tubular Eccentric Moderate tortuosity Moderately angulated (45 – 900) Irregular contour Moderate – heavy calcification Total occlusion (< 3 months) Ostial Bifurcation lesion Thrombus present Note: B 1 = characteristic only; B 2 = 2 or more characteristics
Coronary Angiography Lesion Classification: Coronary Angiographic Outcomes Predictors Based on AHA/ACC Grading System Type C Diffuse Excessive Tortuosity Extremely angulated Total occlusion (> 3 months) Inability to protect major side branch Degenerated vein graft
Current Applicability of Lesion Classification • Mayo Clinic 2004 review of 5000 cases • In hospital MACE by lesion grade: – Type A 1. 2% – Type B 1 1. 1% – Type B 2 2. 2% – Type C 4. 9% Singh: J Am Coll Cardiol 2004; 44: 357 -61
Coronary Angiography Distal Blood Flow/Collateral Classification Based on TIMI Trial TIMI Grade Contrast Flow 0 (No perfusion) Antegrade flow to lesion; no flow beyond occlusion 1 (Penetration with minimal perfusion) Contrast passes beyond lesion but does not opacify distal vessel during cine run 2 (Partial perfusion) Contrast passes obstruction and fills distal vessel. However, rate of filling and/or washout slower than vessel segments outside lesion 3 (Complete perfusion) Contrast passes freely into distal at same visual rate as unaffected adjacent vessels
Adjunctive Pharmacology
“Necessary” Pharmacology • • • Aspirin Clopidogrel/Prasugrel Anti-ischemic Therapy CHF Management if needed STATINS
General Patient Management • Pharmacology helps stabilize patient • Procedure electively only after patient clinically and hemodynamically stable!
Basic Equipment Use
Role of Guide Catheters • • Inject Contrast. Deliver Coronary Devices. Support Delivery of Devices/wires. Measure Arterial Pressure
Guide Catheters • Shapes – Never the same as diagnostics • Sizes – 6 fr. To 9 fr. The larger the shaft the greater the support. (Manufacturers have been unable to make Guides with internal diameters larger than the outer diameter!) • Types – Judkins, Amplatz, Multi-purpose, Xb • Side holes – Useful for RCA, Caution on Left Coronary (Limit coronary flow and injection)
Guide Catheters • Shapes – Never the same as diagnostics • Sizes – 6 fr. To 9 fr. The larger the shaft the greater the support. (Manufacturers have been unable to make Guides with internal diameters larger than the outer diameter!) • Types – Judkins, Amplatz, Multi-purpose, Xb • Side holes – Useful for RCA, Caution on Left Coronary (Limit coronary flow and injection)
Selection of Guide Catheters • Inside diameter determines the ability to inject contrast once equipment in place. – Solutions: Upsize or completely remove balloon from catheter for final pictures. Use monorail balloon catheters. • 7 fr. or 8 fr. Improves visibility and flexibility using simultaneous or kissing balloons or stents in branch disease. (Monorails reduce size Guide Catheter size required)
Left Judkins Sizes Dehmer & Popma: Cathsap III
Left Judkins Manipulation Dehmer & Popma: Cathsap III
Left Judkins Manipulation Dehmer & Popma: Cathsap III
Right Judkins Sizing Dehmer & Popma: Cathsap III
Right Judkins Manipulation Dehmer & Popma: Cathsap III
Right Judkins Manipulation Dehmer & Popma: Cathsap III
Left Amplatz Curve Sizes Dehmer & Popma: Cathsap III
Amplatz Manipulation Dehmer & Popma: Cathsap III
Catheter Pressure Measurement Dehmer & Popma: Cathsap III
Characteristics of Guide Catheters vs. Diagnostics • Relatively larger lumen. • “Stiffer” – Consequence as can “kink” readily. Forward and backward motion as well as rotation often necessary to deliver torque without “kinking” catheter. • Tip Non Tapered. • Tip May be Soft or Radiopaque.
Guiding Catheters • • • Judkins Amplatz Voda XB Multipurpose Williams Kimny El Gamal Arani Radial Shapes
Guide Catheters • Support: • Left Coronary: – Amplatz, XB, L Judkins – Smaller curve allows one to “Amplatzise” left. • Right Coronary: – Amplatz
Guide Catheters • Removing Amplatz Guide from Left Coronary (to avoid Deep-Throating) • Advance and turn counter clockwise to have fall out into ventricle. • Removing from Right Coronary • Turn counter clockwise and withraw.
Guideswire • Tip characteristics: – Shapes – All shapeable, but some retain shape better. The stiffer the tip the greater push to cross a lesion but the greater the risk of perforation. – Stiffness - Floppy, Intermediate, etc. • Shaft Characteristics: – Support – regular, extra support, etc. The greater the support the easier deliverability except in tortuous vessels where stiffness may create friction in the vessel.
Guide Wires • Shaping: • Usual – 30 – 60 degree Hockey Stick configuration. • Circumflex Marginal – “S” bend. • LAD (High Takeoff) Left Judkins configuration.
Guide wires Pearls: – Teflon coated wires increase risk of perforation while they may improve cross ability. Therefore always change out as soon as across lesion to avoid perforation. – High support guide wires may not traverse extreme tortuosity – so may need to cross with low support wire and then exchange. – Wires with graded shaft stiffness transition improves wire passage through tortuosity. – Rotating wire as advanced with balloon/stent backup will improve guide wire steerability and advancement.
Stent Deployment
Stent Deployment • Correct size. • Correct Position. • Complete apposition Before Placing DES be sure no impending surgery
Drug Eluting Stent: Significance of Apposition
DES: Restenosis
Post Procedure Angiography
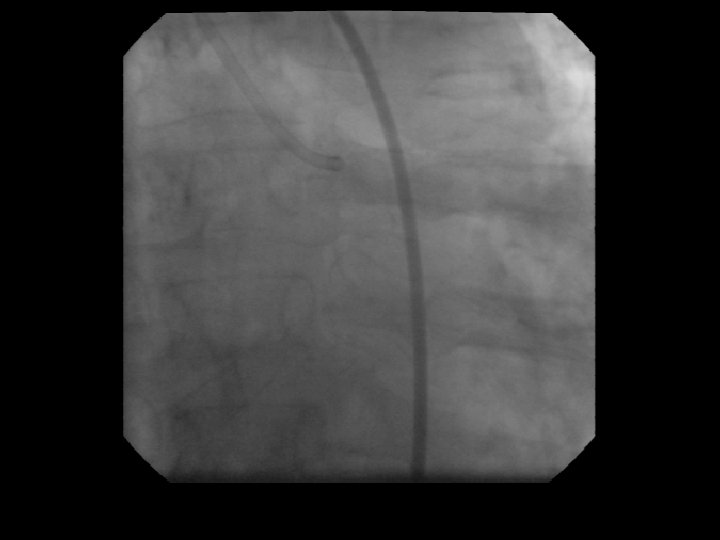
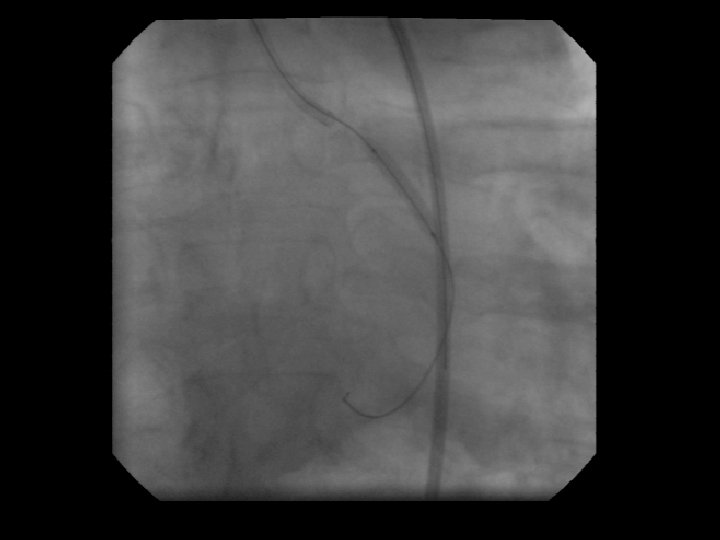
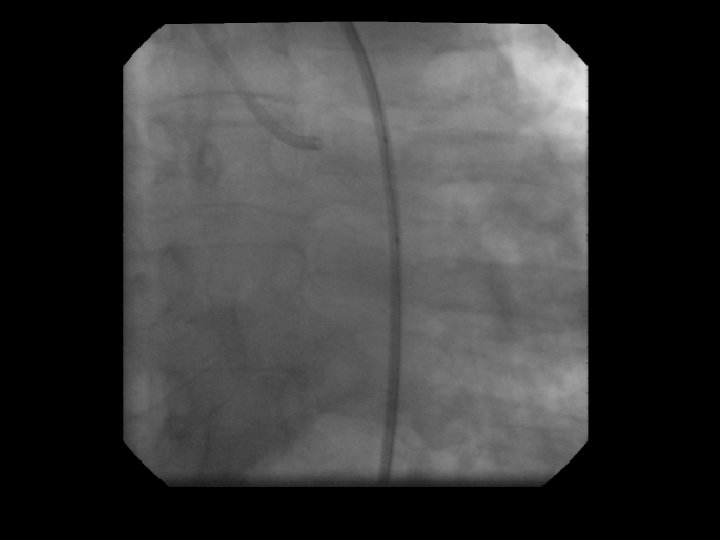
Coronary Dissection
Coronary Dissection
Think first: Use force Last
Compliance • Stent Selection • Follow up
Percutaneous Interventional Techniques: The Basics Conclusions: Careful planning and appropriate use of angiography, pharmacology, basic equipment and procedures techniques can significantly reduce time, radiation and contrast volume while optimizing outcome and maximizing patient safety.