MACROCYTIC ANEMIAS Anemias where the RBC are larger

MACROCYTIC ANEMIAS Anemias where the RBC are larger than normal 1

Macrocytic anemias are classified as megaloblastic & non-megaloblastic 2

Megaloblastic anemia • the most common cause of macrocytic anemia • is due to a deficiency of either vitamin B 12, folic acid (or both). • Pernicious anemia is caused by a lack of intrinsic factor 3

Megaloblastic anemia • associated with defective DNA synthesis • and therefore, abnormal RBC maturation in the marrow (a nuclear maturation defect). 4

Megaloblastic anemia • Primary defect in DNA replication is due to depletion of thymidine triphosphate which leads to retarded mitosis, therefore retarded nuclear maturation. • Cytoplasmic maturation proceeds ahead of nuclear maturation • Nuclear/cytoplasmic asynchrony

Megaloblastic anemia the granulocytic & megakaryocytic maturation are also affected, this leads to pancytopenia 6
 – produced in the stomach » Vitamin")
Vitamin B 12 » Intrinsic factor (IF) – produced in the stomach » Vitamin B 12 & IF complex binds to mucosal cells in the ileum & enters. » B 12 is released from the mucosal cell, » it binds to transport proteins (transcobalamin) in the blood » B 12 is transported to the bone marrow for use or to the liver for storage. 7

VITAMIN B 12 ABSORPTION Mucosal cell 8

9

Requirement » Humans need 3 -5 ug/day of vit B 12 » Since only 70% of dietary B 12 is absorbed, the diet needs to contain 5 -7 ug/day. » Decreased vitamin B 12 therefore results in no conversion of N 5 -methyl THF to THF. Thus, the net result is that d. TMP for DNA synthesis is not made. 10
 is found in meats, eggs, dairy products, liver. »")
Requirement Vitamin B 12 (cyanocobalamin) is found in meats, eggs, dairy products, liver. » Humans need 3 -5 ug/day of vit B 12 » Since only 70% of dietary B 12 is absorbed, the diet needs to contain 5 -7 ug/day. 11

MEGALOBLASTIC ANEMIAS » Therefore, with decreased folic acid, the net result is the same as that for decreased vitamin B 12 – there is decreased conversion of d. UMP to d. TMP, and thus, d. TTP which is required for DNA synthesis. » Defective DNA synthesis may occur when d. UTP gets used in place of d. TTP because there is a great increase in erroneous DNA copying where d. UTP is put in place of d. TTP. » Humans need to get about 50 ug/day of folic acid from the diet 12

Causes of Vit. B 12 deficiency 1. Malabsorption 2. Inadequate intake 3. Inadequate utilisation 13
 Inadequate production of intrinsic factor")
Causes of Vit. B 12 deficiency 1. Malabsorption a) Inadequate production of intrinsic factor pernicious anemia - gastrectomy - atrophy of gastric mucosa b) Inadequate release of vit. B 12 from food c) Terminal ileum disease d) Competition for intestinal B 12 : - bacterial overgrowth e) Defective or absent transport protein (transcobalamin) 14

Causes of Vit. B 12 deficiency 2. Inadequate intake - vegans 3. Inadequate utilisation Drugs 15

PERNICIOUS ANEMIA • • • vitamin B 12, due to a def of IF 60 -70 years, rare before 40 years Auto-immune pathology, parietal cells & IF antibodies 16
- that blocks the binding of vitamin")
Three types of autoantibodies • Type I (75%)- that blocks the binding of vitamin B 12 to intrinsic factor. • Type II - prevent binding of the intrinsic factor –vitamin B 12 complex to its ileal receptor. • Type III (85 -90%) recognize the α & β subunits of the gastric proton pump not specific 17

CLINICAL Anemia with variable severity Mild jaundice Neurological Myelitis => paraplegia. Pyramidal & posterior column lesions. Digestive Glossitis Dyspepsia Diarrhea 18
 » found in most foods, » abundant in green")
Folic acid (pteroyl glutamic acid) » found in most foods, » abundant in green leafy vegetables » eggs, milk, yeast, liver. » destroyed by heat » Absorption occurs in duodenum & jejunum » need about 50 ug/day of folic acid 19

Causes of Folic acid deficiency 1. Inadequate intake 2. Malabsorption 3. Increased requirement 4. Defective utilisation 20

Folic acid deficiency 1. Inadequate intake - diet lacking fresh food; chronic alcoholism, total parenteral nutrition, 2. Malabsorption - small bowel disease - alcoholism 21

Folic acid deficiency 3. Increased requirement - pregnancy, lactation - infancy - chronic hemolysis - hemodialysis 4. Defective utilisation drugs D. Excess urinary folate loss 22

MEGALOBLASTIC ANEMIAS – In both types of deficiency the symptoms include pallor, weakness, lightheadedness, a smooth, sore tongue, and diarrhea alternating with constipation – In vitamin B 12 deficiency, there are neurological disturbances including numbness and tingling of extremities, gait abnormalities, and mental disturbances. » Older theories suggest that the B 12 deficiency leads to a defect in the degradation of propionyl Co. A to succinyl Co. A leading to an accumulation of propionyl Co. A: 23

MEGALOBLASTIC ANEMIA Diagnosis 1. Diagnosis of megaloblastic anemia 2. Establishing the type of deficiency (vit. B 12 and/or folic acid) 3. Establishing the cause of deficiency 24
)")
MEGALOBLASTIC ANEMIAS • Lab findings – Macrocytic, normochromic anemia (MCV=100 -140, MCHC is normal)) – MCH is increased (due to increased cell size) –Hemoglobin & RBC counts are decreased –WBC & platelet counts are decreased 25

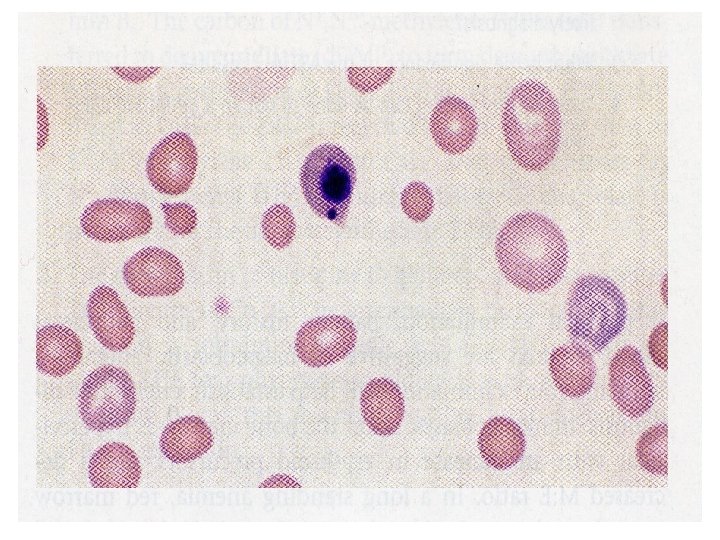
MEGALOBLASTIC ANEMIAS peripheral smear, a triad of findings is commonly seen: oval macrocytes, Howell Jolly bodies (nuclear DNA fragments), hypersegmented neutrophils (5 or more lobes). 26

Peripheral Smear - Megaloblastic Anemia 27 Hypersegmented neutrophil

Macrocytic Anemia MCV > 100 28

Megaloblastic Anemia 29

Howell-Jolly body

MEGALOBLASTIC ANEMIAS peripheral smear, nucleated RBCs, polychromatophilia, The absolute reticulocyte count is decreased because of ineffective erythropoiesis. 31

BONE MARROW PICTURE • • • Hypercellular Megaloblasts Giant band forms Giant metamyelocytes Abnormal megakaryocytes with multilobated nuclei
 abnormal, large, nucleated erythroid precursors, having nuclear-cytoplasmic asynchrony i. e. nuclear")
Megaloblast (vs Normoblast) abnormal, large, nucleated erythroid precursors, having nuclear-cytoplasmic asynchrony i. e. nuclear maturation lags behind that of cytoplasm The nuclei are large, having fine, reticular and open chromatin that stains lightly 34

BONE MARROW-MEGALOBLASTS

36

37

MEGALOBLASTIC ANEMIAS The bone marrow will show hypercellularity, yet there are decreased numbers of all cell types in the peripheral blood (pancytopenia) because of ineffective hematopoiesis & many cells are dying prematurely in the bone marrow. 38

BONE MARROW BIOPSY

Biochemical changes – rise in serun unconjugated bilirubin & LDH 40

Special tests • • • Serum vitamin B 12 assay Schilling test Urinary excretion of FIGLU Serum folate essay Red cell folate essay

MEGALOBLASTIC ANEMIAS In B 12 deficiency –decreased serum vitamin B 12 In folic acid deficiency –decreased serum & RBC folate 42

MEGALOBLASTIC ANEMIAS Specific tests for PA » Gastric analysis – if there is no free HCl after histamine stimulation, this may indicate PA since the same cells that secrete HCl, also secrete intrinsic factor (IF) » Test for antibodies to IF 43

Megaloblastic Anemia Other Labs • Homocysteine – Folate def. • Methylmalonic acid – B 12 def. • Schilling test 44

SCHILLING TEST low 45

MEGALOBLASTIC ANEMIA Endoscopy : –Atrophic gastritis –Intestinal metaplasia 46

Macrocytic anaemia -Non-megaloblastic • • Haemolysis Liver disease Alcoholism Hypothyroidism Aplastic anaemia Myeloproliferative disorders Reticulocytosis
- Slides: 47