Management of cirrhosis Dr Nowlan Selvapatt Consultant Hepatologist












 Alkaline Phosphatase (GGT) (bilirubin) Platelets")


 • If person has chronic liver disease")






 Pharmacological • Consider testosterone supplementation in patients with low")






 • Management of cirrhosis is multisystem – refer to specialist hepatology")
- Slides: 33
Management of cirrhosis Dr Nowlan Selvapatt Consultant Hepatologist Imperial College Healthcare NHS Trust
Overview 1. Understanding the scale of the problem 2. Brief overview of referral pathways 3. Diagnostics in Primary Care 4. Complications of cirrhosis 5. Considerations for Primary Care Management
Understanding the scale of the problem
Increasing Burden of Disease Lancet commission report 2015
Increasing Burden of Disease Lancet commission report 2015
NCEPOD 2013 • 6 month review of 2454 patient notes • Median age of death 56 in females and 58 in males • 112/204 had guidelines for management of patients with ALD • The initial management plan was unclear or inappropriate in one in six (61/363)
NCEPOD – delivery of care
Referral Pathways
Urgency of referrals Incidental radiological finding with compensated disease VS Decompensated cirrhosis or acute deterioation
Why bother referring?
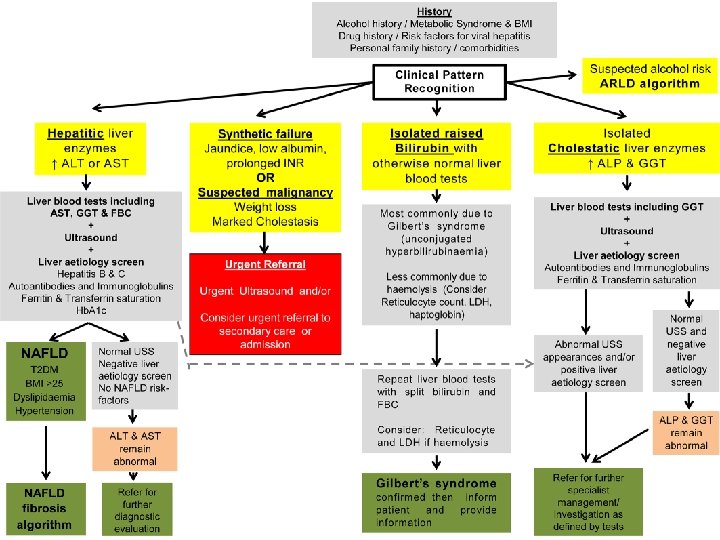
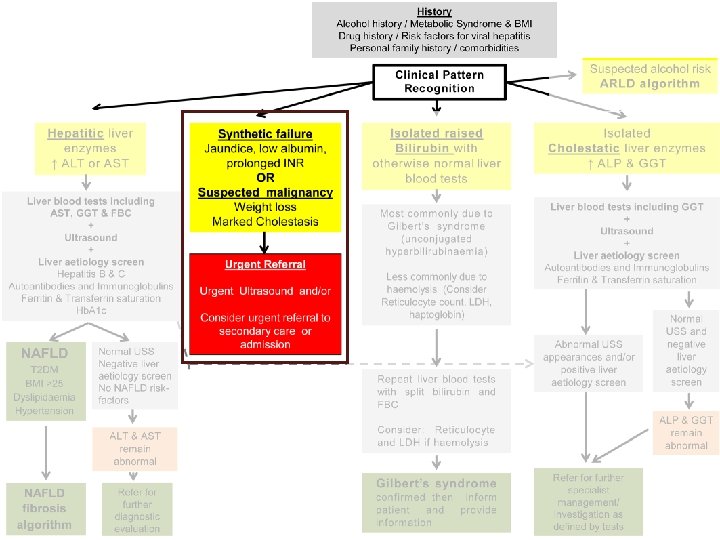
Diagnostics in primary care
The role of the liver
Understanding components of LFTs AST/ALT Albumin Prothrombin time (bilirubin) Alkaline Phosphatase (GGT) (bilirubin) Platelets
Non invasive predictors Adler, Gulbis, Moreno et al. Hepatology 2019
When to suspect cirrhosis - NICE • High risk groups: – Malaise, fatigue, anorexia, nausea, weight loss, muscle wasting, or abdominal pain • If examination identifies – Palpable left lobe of liver, organomegaly – Chronic stigmata of CLD – Features of decompensated disease including abnormal bruising
When to suspect cirrhosis – NICE (2) • If person has chronic liver disease – Low platelets – Raised AST: ALT ratio – Hyperbilirubinaemia – Hypoalbuminaemia – Raised INR
Complications of cirrhosis
Complications of cirrhosis • • • Varices Ascites Encephalopathy Sepsis Sarcopenia/Nutrition/Frailty Extra hepatic organ dysfunction (kidney, heart, adrenal…. )
Sepsis in cirrhosis Bacterial infections in cirrhosis: • leading cause morbidity/mortality in cirrhosis (x 4 MR) Frequency Ø hospitalised cirrhotic patients - 32 -34% Ø hospitalised cirrhotic patients with GI bleeding - 45% Ø vs. hospitalised patients overall 5 -7% • 30 -50% infections remain “culture negative” in cirrhosis Ø SIRS in cirrhosis is atypical *Bajaj et al; Hepatology ’ 12 ‘ 14; Verbake et al; Crit Care ‘ 11; Moreau et al, Gastro ‘ 13
Pathophysiological Changes Seen in frailty Laube et al. Liver Int 2018
Frailty, Sarcopenia and Malnutrition
MDT Approach to frailty Management approaches to frailty Exercise 1. Aerobic exercise 2. Resistance training 3. Prehabilitation program prior to surgery or liver transplantation Nutrition 1. Adequate caloric intake to meet daily requirements 2. Protein supplementation 3. Late night snacks
MDT Approach to frailty (2) Pharmacological • Consider testosterone supplementation in patients with low serum testosterone levels Cognitive • Cognitive training programs including memory, attention and problem‐solving tasks
Primary Care Management
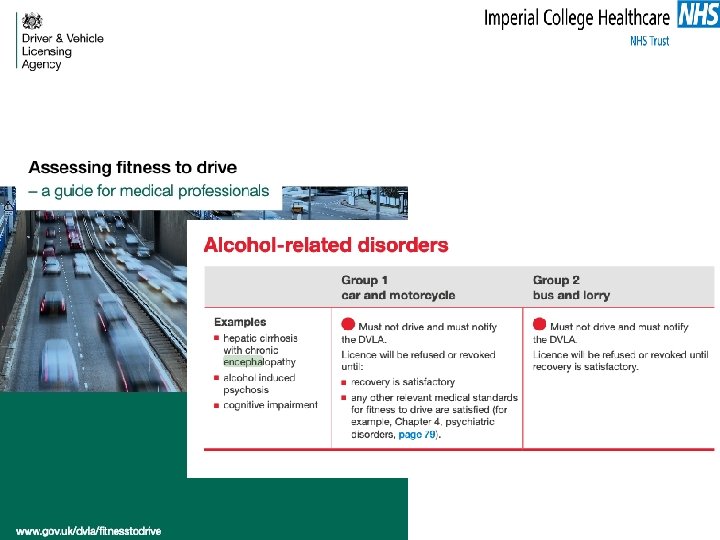
Managing cirrhosis in Primary Care • Education • Healthy eating and Diet • Alcohol consumption and smoking • Driving • Using Medication Safely • Referral to specialty hepatology services
Education https: //www. britishlivertrust. org. uk/wp-content/uploads/44952 Cirrhosis-DL-booklet-Web-compressed. pdf
Diet https: //www. britishlivertrust. org. uk/wp-content/uploads/44951 -DLD-BLT-A 5 -Booklet-webcompressed. pdf
Prescribing
Take home • Identifying cirrhosis can be difficult, diagnosis is often delayed. • Almost half of people with cirrhosis experience no symptoms of liver disease • Liver function tests may be normal or only mildly abnormal • Some people may present with the less specific features of liver disease, for example, fatigue, itch, or loss of appetite
Take Home (2) • Management of cirrhosis is multisystem – refer to specialist hepatology services early • Primary care has an important role within the MDT • Think: – Education – Nutrition – Medications – DVLA