Macau Society of Emergency and Critical Care Medicine






 – Inadequate because of")










 or 3 1(across pump and oxygenator) •")



 – Return part of oxygenated")

 – Shunt part of the")



 Indicated in patients with high bleeding risk • • •")

")












![Monitoring of RCA • [i. Ca] • Total [Ca] to [i. Ca] ratio (<2.](https://slidetodoc.com/presentation_image_h/fbd4cafdd6a40c51153c235bf3557a42/image-43.jpg "Monitoring of RCA • [i. Ca] • Total [Ca] to [i. Ca] ratio (<2.")





- Slides: 49
Macau Society of Emergency and Critical Care Medicine Renal Support during ECMO Dr Yan Wing Wa Department of Intensive Care Pamela Youde Nethersole Eastern Hospital Hong Kong SAR, China 1 February 2013 1
Scope of talk • Why CRRT commonly needed in ECMO? • Types of RRT available during ECMO • Types of connections – Pros and Cons • Regional citrate anticoagulation – Principles – Indications & contraindications – Complications & monitoring – Protocol 2
AKI during ECMO therapy • AKI common complication of shock/hypoxemia – Renal perfusion sacrifice first • Patients are usually in hypercatabolic state – Electrolytes disturbance and acidosis common • Fluid overload is common – May be iatrogenic – Further aggravate the oxygenation status – initial phase – Hinder weaning of ECMO – recovery state • Complication of ECMO – e. g. intravascular hemolysis with kidney impairment 3
Fluid overload • Respiratory failure VV-ECMO preferred • First few days – SIRS with leaky capillaries, decrease effective circulating volume though lung congestion – IVC collapse with sudden dec. in ECMO flow further decrease in Sp. O 2 “Circuit shaking” – Treatment: dec. ECMO speed and slowly turn up again AND give fluid – The above process may be repeated many times – Aggravate the fluid overload – Difficult to detect because no desaturation or accept low Sp. O 2 – Beware of daily I&O, CXR and echocardiography 4
Venous O 2 saturation Mixed blood O 2 saturation ECMO flow as % of total blood flow 5
Fluid overload • CXR remains diffuse air space shadows – Difficult to detect resolution of underlying pneumonia – Viral pneumonitis recovers within a few days only • Negative fluid balance by ultrafiltration or hemofiltration – Lasix bolus or infusion may not work • Aggressive fluid restriction after the first few days • Try to cut down the duration of ECMO as much as possible – ECMO complications increase with time (not linear but exponential) • Then monitor disease progression by assessing CXR, changes in lung mechanics, Sp. O 2, ECMO flow needed, BP, pulse, temp, inotropes needed, 6
Types of RRT possible with ECMO • Peritoneal dialysis (PD) – Inadequate because of high metabolic rate – Inherent complications of PD • Extracorporeal circuit – Hemofilter only – CRRT machines 7
Nomenclature • RRT – Arterial line lead to renal filter/dialyser – Venous line from renal filter/dialyser • ECMO – Venous line lead to oxygenator – Arterial line from oxygenator back to patient 8
CRRT • Separate CRRT circuit – Less complication related to ECMO – Access problem • No site • Risk of air embolism during insertion • Difficult venepuncture when ECMO is in-situ – May need to dec. pump flow transiently during insertion • CRRT circuit attached on to the EVMO circuit 9
Extracorporeal flow needed Separate cannulae needed or Avalon cannula 1000 0 ae siz e r Inc 1000 Flow ml/min ng asi ul ann c f eo ECMO ECCO 2 R 100 IHD CRRT MARS 10 Plasmaphoresis Regional citrate anticoagulation possible 10
1 3 2 11
Possible types of connection • 1 2 • 2 1 • 1 3 • 3 1 • 2 3 • 3 2 12
Important points • Region 1: – Negative pressure – Once leak, air suck into circuit • Pump fails immediately and circuit stops if massive • Gas embolism if partial and prolonged • Some centres call this region “Virgin area” and cannot be touched • Cardiohelp no connection port in this region • Region 2: – Highest positive pressure – Once leak, blood out – Cardiohelp very much reduced because pump incorporated into oxygenator • Region 3: – Positive pressure, less than region 2 – Once leak, blood out • Oxygenator: – Also as a filter for gas and clot 13
Possible types of connection for Cadiohelp • 2 3 • 3 2 14
Types of RRT • Haemofilter only – 2 3 or – 2 1 or – 3 1 possible • CRRT machine – CRRT machines • Prisma: +ve pressure not allowed in a-limb – Otherwise long alarm – Only 1 2 or 1 3 possible • Prsimaflex: ok but needs adjustment – Haemodialysis machines • Ok but needs adjustment 15
Hemofilter alone - Across oxygenator 2 3 • Not suitable for PMP type of oxygenator – Maquet - Quadrox D, Medos – Hilite 7000 LT, Sorin – Lilliput 2, Eurosets – Eurosets ECMO, Terumo – Capiox EMS – Because of low pressure gradient across oxygenator may be inadequate driving pressure for blood flowing through hemofilter • Coiled Silicone membrane, e. g. Medtronic Avecor 4500 – High resistance and therefore big pressure drop 16
Pressure drop across Quadrox. D oxygenator 17
Hemofilter alone - 2 1 (across pump) or 3 1(across pump and oxygenator) • Feasible but • Connection over the pre-pump (negative pressure) – Increase risk of circuit gas embolism • Circuit stop – Patient gas embolism • Can be rapidly fatal • Simple but need very close monitoring, e. g. in OT setting • Measure ultrafiltration volume – Even guarded with volumetric pump • Slow continuous ultrafiltration (SCUF) or • Continuous hemofiltration + replacement solution (somewhere) 18
Hemofilter alone • Not advisable “possible” in ICU setting – Volumes not accurate (need to measure Uf volume) • Measurement involve error which become significant over time – Circuit/air embolism – Need of very close monitoring – Consumable availability 19
oxygenator 1 2, 2 1, 1 3, 3 1 2 3 or 3 2 • CRRT flow maintained by internal motor of machine – Not influenced by access or return point pressures • Clearance rate much higher than SCUF – 20 -25 ml/kg/h for RRT – >50 ml/kg/h for High Volume Hemofiltration (HVHF) 20
CRRT machine across oxygenator 1 2, 2 1, 1 3, 3 1 • Risk of circuit and gas embolism • Not possible in Cardiohelp • Not advisable 21
CRRT machine across oxygenator • Post-oxygenator Pre-oxygenator (3 2) – Return part of oxygenated blood flow back to preoxygenator • More flow through oxygenator – Oxygenator act as an additional bubble trap in case air get into the CVVH circuit – Less systemic arterial embolism for VA-ECMO – Increase risk of oxygenator thrombosis • May increase need of change of oxygenator & • Associated risk related to oxygenator change and COST • Better CRRT circuit anticoagulation is preferred 22
Oxygenator • Oxygenator itself as a filter for clot and gas 23
CRRT machine across oxygenator • Pre-oxygenator Post-oxygenator (2 3) – Shunt part of the deoxygenated blood to patient blood – Decrease ECMO efficiency, may need increase pump flow • May not be possible if patient’s oxygenation status is very marginal & pump flow is pushed to maximum already • Inc. risk of patient embolism – Significant if VA-ECMO – Less significant if VV-ECMO (lung as filter) • Beware of PFO because of pulmonary hypertension 24
ECMO circuit priming with normal saline • Priming volume ~500 ml as compared with normal blood volume ~5, 000 ml • Hemodilution – Lower hematocrit – Lower Ca++ – Lower drug levels – Inc. in volume of distribution – Except Na+ and Cl- • Consider priming with Lactated Ringer solution 25
CRRT Anticoagulation • No anticoagulation if patient is contraindicated for systemic anticoagulation • ECMO & the attached CVVH circuit still can last for days without anticoagulation – Bioline coating (Maquet-Quadrox D) of cannulae, tubing and oxygenator – Both Cardiohelp and Rotaflow – Try not to use protamine to reverse anticoagulation • decrease effect of Bioline coating 26
CRRT Anticoagulation • Regional citrate anticoagulation to CVVH circuit only, not the ECMO circuit • Beware of contraindication – hepatic impairment (hypoxic hepatitis, especially patients with high INR and hypoglycemia) • Good for other causes of bleeding tendency • Excellent anticoagulation property – Less effect on oxygenator and – patient 27
Regional citrate anticoagulation (RCA) Indicated in patients with high bleeding risk • • • Thrombocytopenia Coagulopathy Pericarditis Recent surgery with bleeding complications Recent surgery after which bleeding would be very dangerous – Brain or eye surgery – Vascular or cardiac surgery 28
Citrate calcium interaction Citrate + i. Ca Calcium citrate Biologically inactive Measurable as total calcium 29
RCA • Citrate binds with i. Ca to form Ca-citrate (partially removed in ultrafiltrate) • Circuit [i. Ca] decreased to ~ 0. 3 mmol/l • Systemic [i. Ca] normalized by – Mainly by dilution of extracorporeal blood – Calcium supplement is needed in long term because of extra loss in ultrafiltrate as Ca citrate – Liberation of Ca from returned Ca-citrate • Citrate 3 - 3 HCO 3 - (buffer) 30
31
Longer Filter Life 32
Less Clotting 33
Less Inflammatory Activation 34
Less Transfusion 35
RCA Contraindications • Significant liver impairment • Massive blood transfusion – Relative contraindication only 36
Gl uc on eo ge n si s Citric acid cycle Phosphoenolpyruvate id Lip hes t syn is Pyruvate Endogenous citrate Oxidation Citrate Malate NAD+ H 2 O NADH O 2
Total to ionized calcium gap • If high rate of citrate infusion and/or hepatic dysfunction – Accumulation of calcium citrate (total) – Progressive decrease in systemic i. Ca level – Indicative of citrate accumulation/toxicity 38
mmol/ L Calcium Gap
Calcium Gap
41
Complications of RCA • Related to calcium chelation/replacement Hypocalcaemia Hypercalcaemia – Skin necrosis due to extravasation • Related to citrate metabolism Metabolic alkalosis Metabolic acidosis • Related to sodium content Hypernatraemia Hyponatraemia • Related to formulation – Electrolytes imbalance – Haemolysis 42
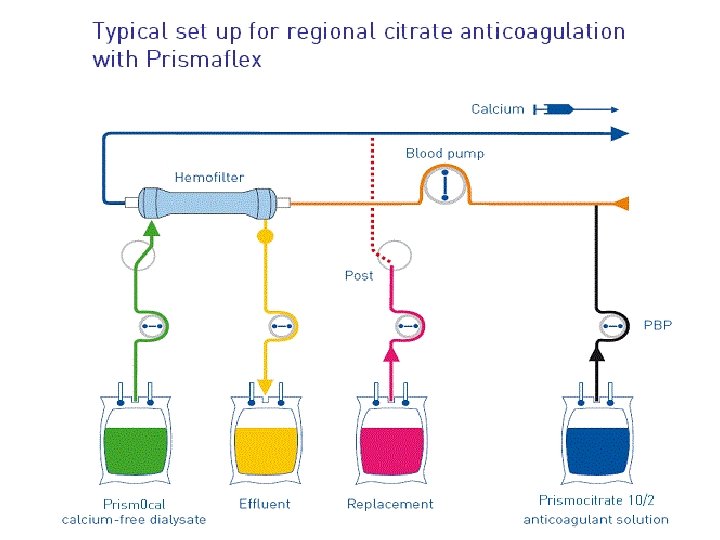
Monitoring of RCA • [i. Ca] • Total [Ca] to [i. Ca] ratio (<2. 5) • Metabolic acidosis & alkalosis – ABG • Sodium overloading (tri-sodium citrate/ACD -A)) – Body fluid status – [Na+] • Phosphate & Magnesium level 43
45
46
47
Conclusion • Why CRRT commonly needed in ECMO? • Types of RRT available during ECMO • Types of connections – Pros and Cons • Regional citrate anticoagulation – Principles – Indications & contraindications – Complications & monitoring – Protocol 48
Thank you for your attention. 49