Christian Medical College Accident Emergency Care in Vellore


 • Founded by Ida S. Scudder ▫ An")
 •")




")




 Census of India 2011. District Census")
- Slides: 15
Christian Medical College: Accident & Emergency Care in Vellore, India Elizabeth Lothamer, KUSON N 4
• Vellore, Tamil Nadu – India ▫ Population - 484, 690 (Census of India 2011) • Religious Breakdown of Vellore � 70% Hindu � 24% Muslim � 5% Christian �Less than 1% �Buddhist �Sikh �Jain �Other *Map of India with marker on Vellore
Background of Christian Medical College (CMC) • Founded by Ida S. Scudder ▫ An American Missionary • Est. 1900 – 1 bed clinic to serve women • 1902 – grew to 40 bed clinic to serve women and children • Present Day - over 2, 800 beds ▫ (4 x bigger than KU) *Ida S. Scudder, 1870 -1960 • Accredited by the National Accreditation Board for Hospitals (NABH) • Non-government, private, interdenominational Christian organization • Serves people from all over India
Accident & Emergency Department • 44 bed unit • 1 trauma bay (stable) • 3 open bays • Ratios ▫ Bay 1 -3: 10 beds � 2 nurses & 1 doctor ▫ For general emergencies ▫ Trauma Bay: 7 beds ▫ For all type one emergencies ▫ Unstable ▫ Resuscitation Room • 1 resuscitation room *Main entrance to emergency department � 1 nurse for 4 patients. 2 doctors � 5 -6 patients, 3 nurses, 2 doctors
Accident & Emergency Clinical Objectives • Identify the main causes for emergency room visits at CMC and compare to those seen at The University of Kansas Health System (TUKHS) • Identify the treatment process of the emergent patient at CMC • Discover the flow of patients and how the system functions under stress • Determine safety hazards in terms of patient care and the solutions that are being done to reduce them • Identify costs associated with care and it’s impact on clinical decision making *Crash cart located in the resuscitation room
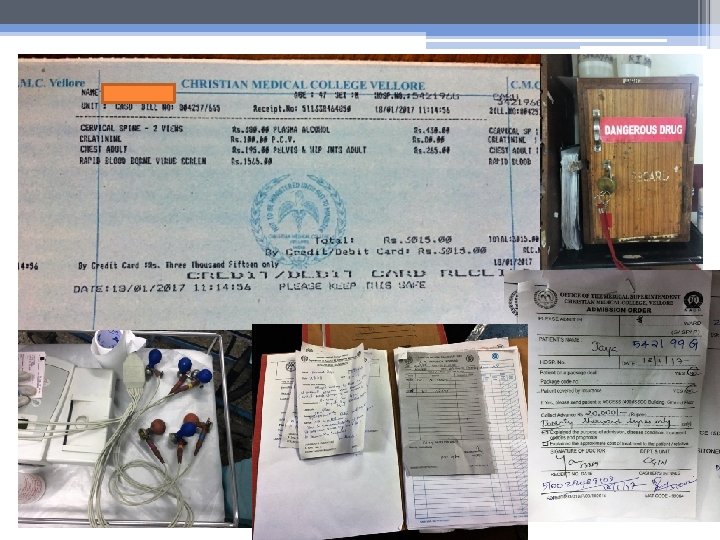
Care of the Accident & Emergency Patient • Top 5 primary complaints ▫ ▫ ▫ Trauma (two-wheeler accidents, pedestrian vs. auto) Cardiac emergencies (HTN, CHF, rheumatic heart disease) Asthma & COPD exacerbations (pollution) Uncontrolled fever (typically GI or URI origin) Severe anemia • Treatment Process ▫ All patients are triaged upon arrival and receive an acuity rating �Level 1 – resuscitation room �First 4 hours of care free of charge for these patients �Level 2 – bay 1 through 3 �Level 3 – referred to outpatient clinic ▫ Emergency staff is conscious to the cost of care – utilize clinical diagnosis and then support with investigation to reduce cost �Average cost of care is 3, 000 rupees ($46 USD) – average income of CMC patient is 15, 000 rupees a month ($231 USD) �Additional costs incur for pharmaceuticals, diagnostic testing, radiographic imaging, and procedures performed
Care of the Accident & Emergency Patient • Flow of Patients ▫ 180 -200 pts/day � 100 -110 admitted ▫ Consider a stay greater than 12 hours in bays 1 through 3 over-stays �greater than 4 hours in the resuscitation room ▫ Bay average is 6 – 8 hours • Patient Safety and Delays of Care ▫ Limited Emergency Medical Services – ambulances are for transport, not for emergent stabilization or resuscitation (witnessed two DOAs) ▫ Infection control risk �Open units �Limited access for hand washing ▫ Limited Resources � 1 portable X-Ray, 1 ultrasound machine, 1 cat scanner. *Brought Dead Certificate �Paper charting – information uploaded to computers after patient is discharged �Discussion with family on cost of care – pick and choose what they can afford
Interventions and Strategies to Reduce Emergencies • Individual ▫ Increased access to primary care facilities �CONCH, CHAD, RHUSA ▫ Utilization of public health nursing for primary prevention and education in the villages �Fever management, clean drinking water education, dietary habit analysis, etc. ▫ Screenings provided in village clinics �HTN, anemia, diabetes, etc. • Community ▫ Emergency Department will teach first aid management and injury prevention to schools, colleges, factories, businesses, and more. �CPR, fracture stabilization, emergency preparedness, etc. ▫ Emergency medical services are very limited at the community level. Many patients self-present to the unit after trying home remedies.
Interventions and Strategies to Reduce Emergencies • System ▫ The World Health Organization (WHO) �Currently working with government organizations in India to improve road safety �Current laws are in place but they are not widely enforced �“The Global status report on road safety 2013 estimates that more than 231, 000 people are killed in road traffic crashes in India every year” (Kansla, 2017) �WHO hopes to accomplish: �Increased road traffic violation fines �More strict helmet laws ▫ Focus shift from communicable to non-communicable diseases �More government programs are being initiated to address the increase in non-communicable diseases like HTN, diabetes, etc.
*Family of 4 rides twowheeler *Blood pressure screening *Anemia screening *Busy morning commute
Conclusions & Suggestions • Conclusions ▫ A large problem in India is overpopulation �Creates concern when it comes to health care resources ▫ Must focus on primary prevention to ensure hospitals do not get over-run �When the Emergency Department starts to get over-ran the staff must rely on their team members and protocols in place in order to make things run smoothly • Suggestions ▫ The emergency department needs to expand in order to accommodate the mass intake the hospital experiences (44 unit beds for 2, 800 inpatient beds) ▫ Increased staffing in order to make safer nurse: patient ratios ▫ Updated equipment ▫ Quicker cost analysis and management in order to reduce care delays
Most Profound Clinical Experience • A double edged sword ▫ Staff maintains a diligent awareness to cost of care ▫ One patient on admittance was pronounced brain dead �The team decided not to intubate �Would not be a noble use of the family’s money �Discharged the patient to home to pass away with family ▫ Another patient on admittance had a skull fracture and was actively bleeding into his brain. �He had a 70% chance of making a livable recovery �Quality of life was unable to be determined. �Their was major delay in whether or not to perform surgery because of the discussion with family �After a significant amount of time had passed the family decided to pay for the surgery �Since it took hours to decide, the patients status had worsened and his odds of success were now worse ▫ I saw the consideration of cost be therapeutic for one patient and detrimental for another, creating a double edged sword phenomena
Most Profound Cultural Experience • The people *Girl from the village daycare ▫ I have never felt more welcomed in a foreign place ▫ I could not speak the language but through gestures, touch, and smiles I was able to connect with the people in a profound way ▫ Truly happy to invite us into their homes and wanted to share all they had ▫ The hospitality of Vellore, India is something of true *Woman from the village of beauty that I will forever Melminnal cherish
References Directorate of Census Operations Tamil Nadu (2011) Census of India 2011. District Census Handbook Vellore. 34, 1 -432. Retrieved from: http: //www. censusindia. gov. in/2011 census/dchb/3304_PART_B_D CHB_VELLORE. pdf Vellore Christian Medical College Foundation, Inc. (2017) Humble yet bold beginnings. Christian Medical College. Retrieved from: https: //www. vellorecmc. org/who-we-are/history/ World Health Organization (2017) Violence and injury prevention: road safety in India. World Health Organization. Retrieved from: http: //www. who. int/violence_injury_prevention/road_traffic/coun trywork/ind/en/