LIU Chuan Yong Department of Physiology Medical School
")










 12")






")












 = represent 1/3 of total")








 • Emphysema (肺气肿) •")




 (wks) 28~30 >70")






- Slides: 55
LIU Chuan Yong 刘传勇 Department of Physiology Medical School of SDU Tel 88381175 (lab) 88382098 (office) Email: liucy@sdu. edu. cn Website: www. physiology. sdu. edu. cn 1
Chapter 3 Elastic Properties of the Respiratory System 2
Reference - Textbook P 29 – 40 P 210 - 218 P 471 – 475
Reference – Course Website 4
An Overview of Key Steps in Respiration 5
Key Steps in Respiration • Ventilation: Movement of air into and out of lungs • Gas exchange between air in lungs and blood • Transport of oxygen and carbon dioxide in the blood • Internal respiration: Gas exchange between the blood and tissues 6
Newborn RDS : Signs and Syndrome • Baby Aldridge – Premature infant (28 weeks gestation) – Breathing very fast – Dyspnea • Chest was indrawing with each breath • Making a grunting sound – Question • The mechanism? • Treatment and prevention 7
Outline • Part I Intrapleural Pressure and Mechanism of the Ventilation • Part II Lung Compliance • Part III The Effect of Disease 8
Part I Intrapleural Pressure and Mechanism of the Ventilation 9
Ventilation • Occurs because thoracic cavity changes volume • Insipiration uses external intercostals and diaphragm • Expiration • passive at rest • uses internal intercostals and abdominals during severe respiratory load • Breathing rate is 10 -20 breaths / minute at rest, 40 - 45 at maximum exercise in adults
Mechanisms of Breathing: How do we change the volume of the rib cage ? To Inhale is an ACTIVE process • External Intercostal Muscles • Diaphragm Rib Cage Spine Intercostals Rib Contract to Lift Contract Diaphragm Volume Ribs Volume Both actions occur simultaneously – otherwise not effective 11
Flail Chest (连枷胸) 12
Pleura 13
• Pleural fluid produced by pleural membranes –Acts as lubricant –Helps hold parietal and visceral pleural membranes together 14
Intrapleural Pressure 15
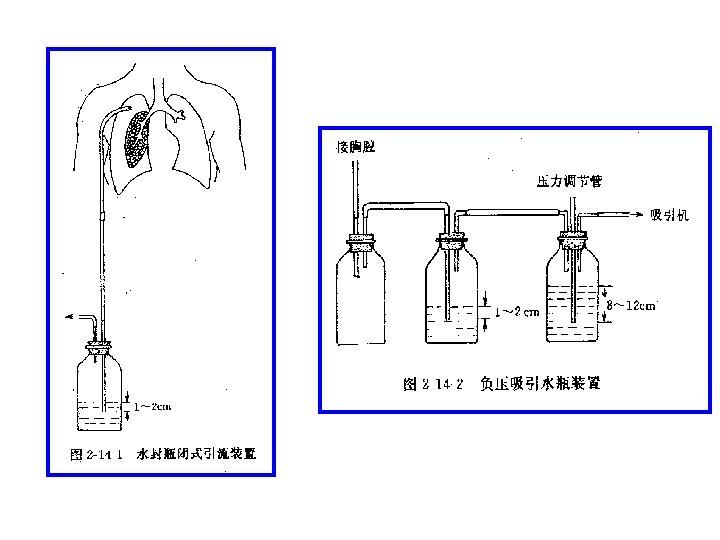
Penumothorax 16
Penumothorax
Alveolar Pressure Changes During Respiration 20
Principles of Breathing Functional Unit: Chest Wall and Lung Follows Boyle’s Law: Pressure (P) x Volume (V) = Constant Conducting Airways Lungs Pleural Cavity Gas Exchange Very small space Maintained at negative pressure Transmits pressure changes Allows lung and ribs to slide Chest Wall (muscle, ribs) Pleural Cavity Diaphragm (muscle) Imaginary Space between Lungs and chest wall 21
Principle of Breathing Follows Boyle’s Law: PV= C At Rest with mouth open Pb = Pi = 0 Pb A Airway Open Pi CW PS D 1 22
Principle of Breathing Follows Boyle’s Law: PV= C At Rest with mouth open Pb = Pi = 0 Inhalation: - Increase Volume of Rib cage - Decrease the pleural cavity pressure - Decrease in Pressure inside (Pi) lungs CW Pb A Airway Open Pi PS D 2 23
Principle of Breathing Follows Boyle’s Law: PV= C At Rest with mouth open Pb = Pi = 0 Inhalation: Pb A Airway Open - Pb outside is now greater than Pi - Air flows down pressure gradient - Until Pi = Pb CW Pi PS D 3 24
Principle of Breathing Follows Boyle’s Law: PV= C Pb At Rest with mouth open Pb = Pi = 0 A Airway Open Pi Exhalation: Opposite Process - Decrease Rib Cage Volume CW PS D 4 25
Principle of Breathing Follows Boyle’s Law: PV= C At Rest with mouth open Pb = Pi = 0 Pb A Exhalation: Opposite Process - Decrease Rib Cage Volume CW - Increase in pleural cavity pressure - Increase Pi 5 Airway Open Pi PS D 26
Principle of Breathing Follows Boyle’s Law: PV= C At Rest with mouth open Pb = Pi = 0 Pb A Exhalation: Opposite Process - Decrease Rib Cage Volume CW - Increase Pi - Pi is greater than Pb - Air flows down pressure gradient - Until Pi = Pb again 6 Airway Open Pi PS D 27
28
Resistance of the Ventilation • Elastic Resistance – Determined by the Compliance – Lung and Thoracic Cage Compliance • Inelastic Resistance – Airway Resistance 29
Part II Lung Compliance 30
Ø Change in lung volume for each unit change in transpulmonary pressure = stretchiness of lungs Ø DV/DP Ø Transpulmonary pressure is the difference in pressure between alveolar pressure and pleural pressure.
Ø There are 2 different curves according to different phases of respiration. Ø The curves are called : Ø Inspiratory compliance curve Ø Expiratory compliance curve Ø Shows the capacity of lungs to “adapt” to small changes of transpulmonary pressure. Ø Hysteresis (滞后现象)
Compliance of lungs occurs due to elastic forces. A. Elastic forces of the lung tissue itself B. Elastic forces of the fluid that lines the inside walls of alveoli and other lung air passages Elastin + Collagen fibres Surface Tension
Conclusion of this experiment: Experiment: Tissue elastic forces (A) = represent 1/3 of total lung elasticity Fluid air surface tension (B) = 2/3 of total lung elasticity. Ø Ø Ø By adding saline solution there is no interface between air and alveolar fluid. (B forces were removed) surface tension is not present, only elastic forces of tissue (A) Transpleural pressures required to expand normal lung = 3 x pressure to expand saline filled lung.
Øwater molecules are attracted to one another. ØThe force of surface tension acts in the plane of the air-liquid boundary to shrink or minimize the liquid-air interface ØIn lungs = water tends to attract forcing air out of alveoli to bronchi = alveoli tend to collapse (!!!) Elastic contractile force of the entire lungs (forces B)
Ø Surface active agent in water = reduces surface tension of water on the alveolar walls Pure water (surface pressure) 72 dynes/cm Normal fluid lining alveoli without surfactant (surface pressure) 50 dynes/cm Normal fluid lining alveoli with surfactant 5 -30 dynes/cm
Pulmonary surfactant • Phospholipid produced by alveolar type II cells. • Develop at 24 weeks’ gestation • Produces surfactant at 34 weeks • Lowers surface tension. – Reduces attractive forces of hydrogen bonding – by becoming interspersed between H 20 molecules. 37
Ø “The pressure inside a balloon is calculated by twice the surface tension, divided by the radius. ” Ø Pressure to collapse generated by alveoli is inversely affected by radius of alveoli Ø Ø the smaller a bubble, the higher the pressure acting on the bubble Smaller alveoli have greater tendency to collapse
Effect of Surface Tension on Alveoli size Air Flow Expand Collapse 39
Surfactant prevents alveolar collapse 40
Physiology Importance of Surfactant • Reduces surface tension and elastic recoil, – making breathing easier • Reduces the tendency to pulmonary edema • Equalize pressure in large and small alveoli • Produces hysteresis, which “props” alveoli open 41
ØThe compliance of lungs + thorax = 1/2 of lungs alone.
Part III The Effect of Disease • Lung fibrosis (肺纤维化) • Emphysema (肺气肿) • Respiratory Distress Syndrome (RDS) of the Newborn (新生儿呼吸窘迫综合症) 43
Lung fibrosis • The lungs are stiffened – By the laying down of collagen and fibrin bundles • Compliance is reduced 44
Emphysema • Destroy of the parenchyma – Less elastic recoil • Compliance increase 45
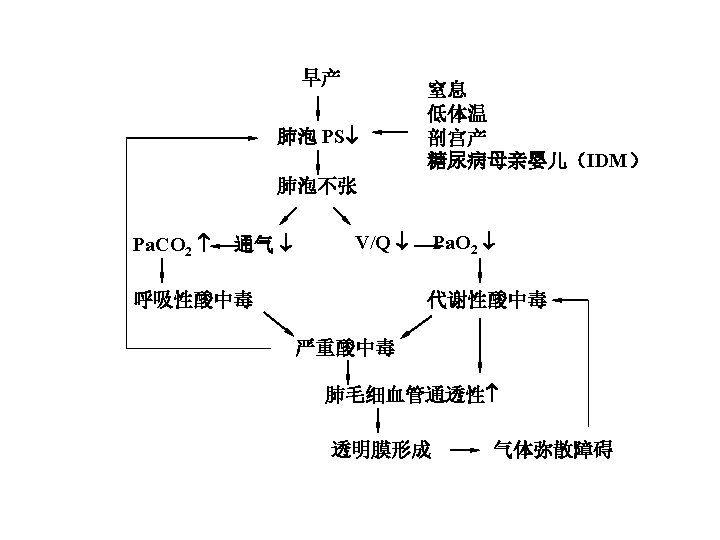
Newborn RDS : Signs and Syndrome • Baby Aldridge – Premature infant (28 weeks gestation) – Breathing very fast – Dyspnea • Chest was indrawing with each breath • Making a grunting sound – Question • The mechanism? • Treatment and prevention 46
Newborn RDS • • Most common respiratory illness in NICU Occur in premature neonate Surfactant deficiency Risk factors – Asphyxia (窒息) – Male – Acidosis – DM mother
Relationship between Gestational Age and RDS Morbidity gestational age morbidity (%) (wks) 28~30 >70 31~32 40~55 33~35 10~15 >36 1~5
collapsed alveoli filled with hyaline membranes
Chest X-ray • Ground glass appearance • Reticulogranular • air bronchograms
diffuse and symmetrical ground glass infiltrates
• Reticulogranular with air bronchograms
Treatment: Surfactant Replacement Before PS treatment After PS treatment
Home Work:Case Study – Mechanics of Breathing. pdf – Pulmonary Structure and Lung Capacities. pdf – Pneumothorax. pdf 55