HISTOSMINAIRE CONJOINT Universite d Montral Universit Mc Gill




 Nov. 04 March. 05")


 of breast. n Differential diagnosis n")
























 – Require extensive")




- Slides: 54
HISTOSÉMINAIRE CONJOINT Universite dé Montréal/ Université Mc. Gill October. 25 th 2006 Saeeda Almarzooqi R 3
Clinical history A 91 year old lady with right breast mass.
Clinical history n June 2004 : – Rt. Breast mass of two weeks duration – U/S: cystic lesion – FNA: benign cyst contents. n Nov. 2004: – Increase in size of mass – U/S: cystic lesion – FNA: foamy macrophages, inflammatory cells.
Clinical history n March. 2005 – Increase in size – U/S – Lumpectomy
Ultrasound of specimen June. 04 ( cyst 4 cm) Nov. 04 March. 05
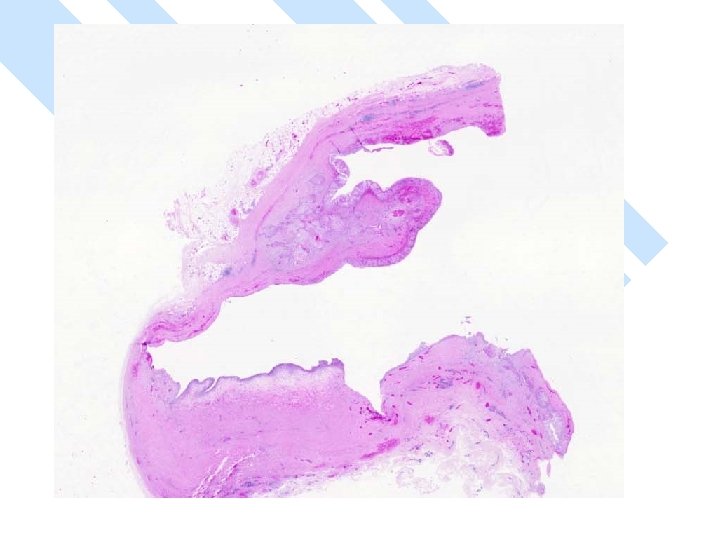
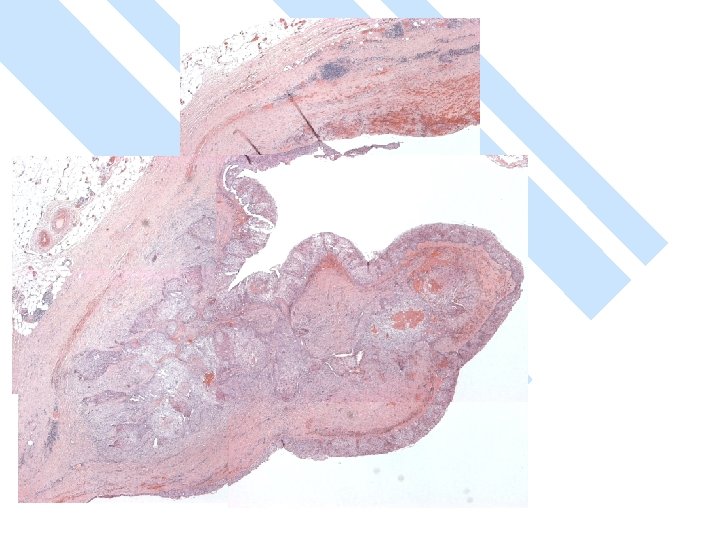
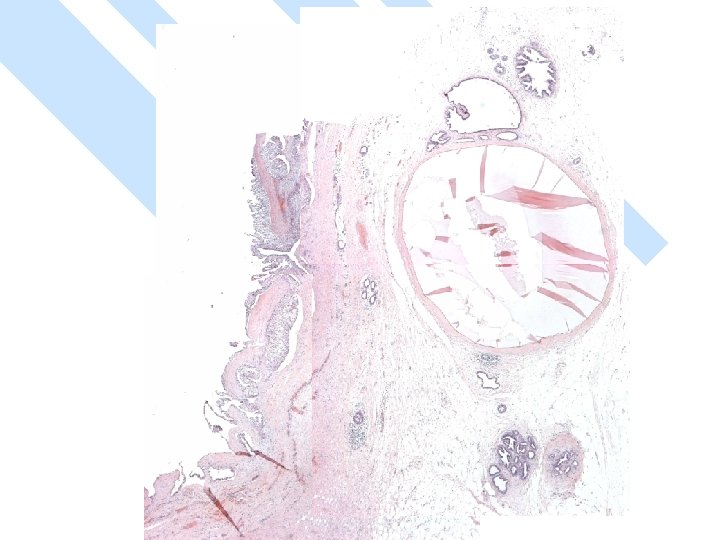
Gross: -A ruptured cyst with attached breast tissue measuring 8. 5 x 6 x 2. 8 cm - area of hemorrhage in cyst wall
DIAGNOSIS
Points of discussion Primary Squamous cell carcinoma (SCC) of breast. n Differential diagnosis n – Metaplastic carcinoma of breast. – Metastatic carcinoma. – Extension of skin SCC. n Role of FNA of breast cysts in diagnosis of malignancy.
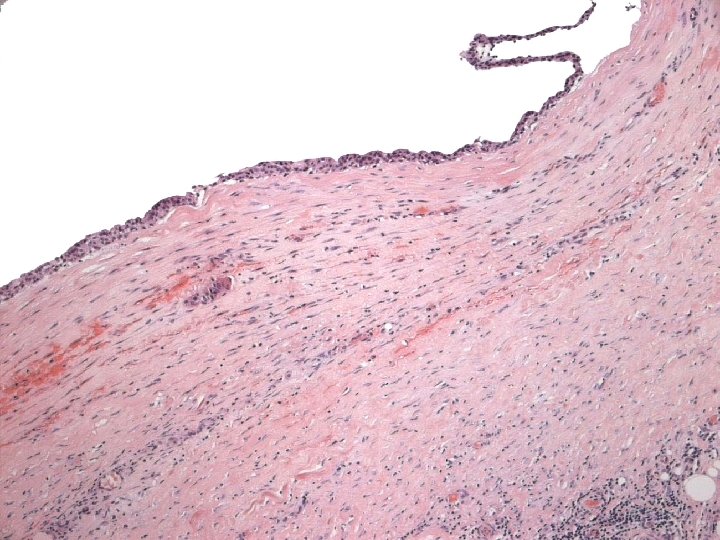
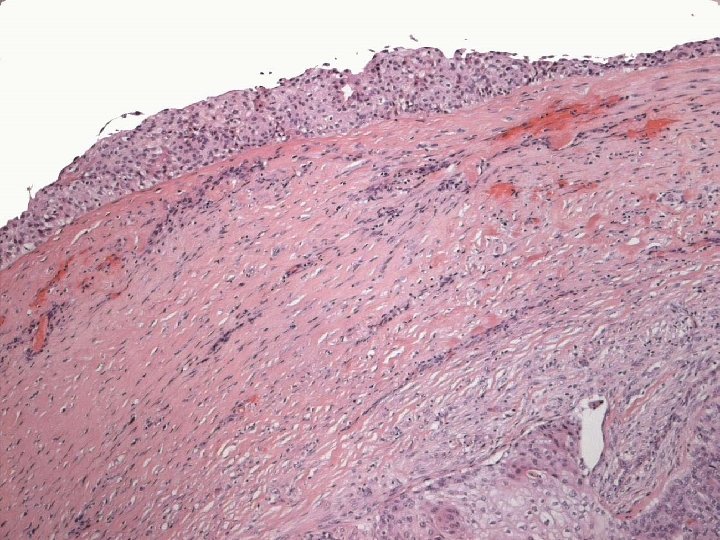
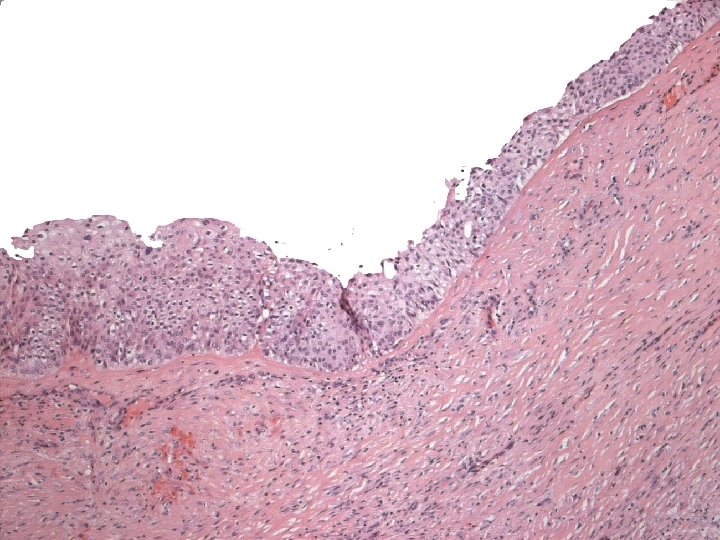
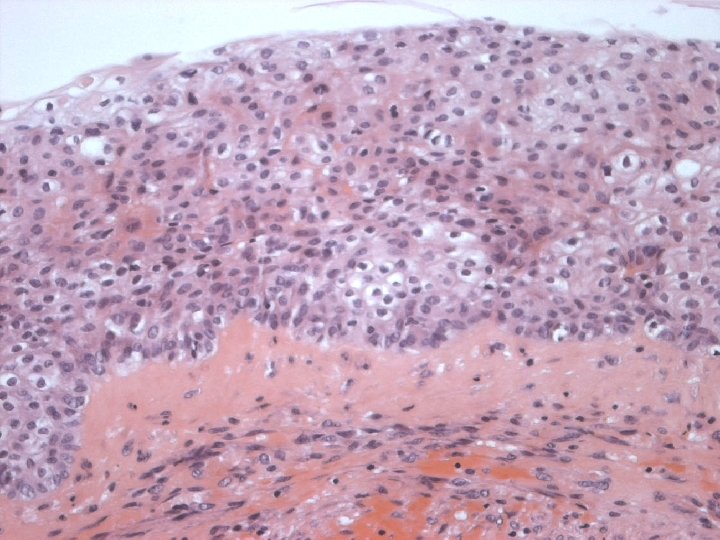
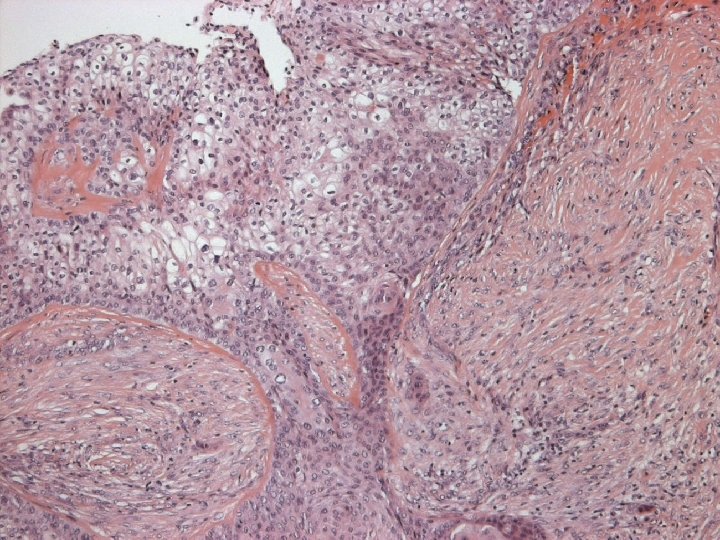
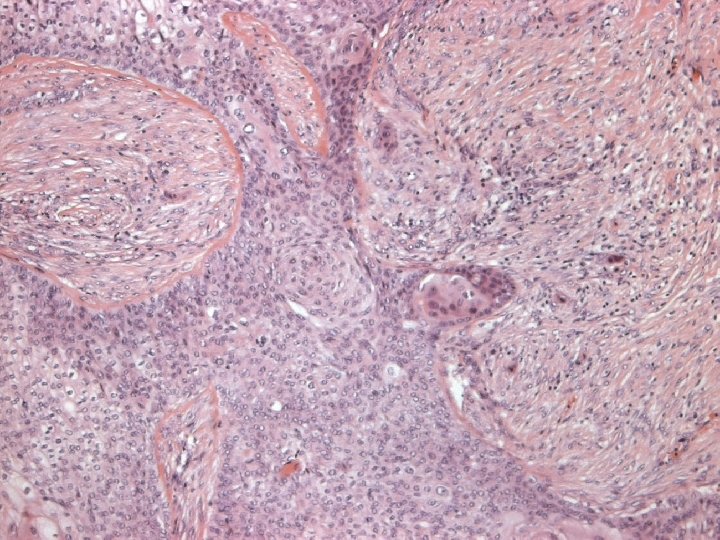
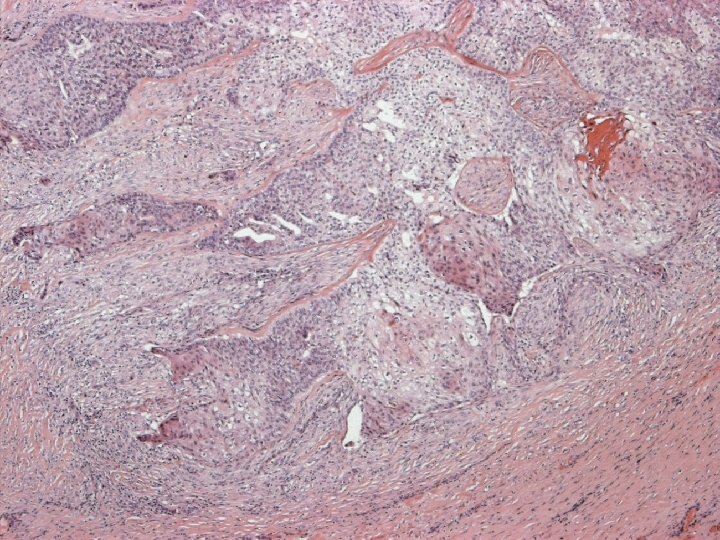
Primary Squamous cell carcinoma A breast carcinoma entirely composed of metaplastic squamous cells that may be keratinising, non-keratinising or spindled; Exclude extension from skin and metastases. (WHO. 2003) Characterised by origin from squamous metaplasia in cyst, duct or both.
Classification of metaplastic carcinoma n Purely epithelial – Squamous » » » Large cell keratinizing Spindle cell Acantholytic – Adenocarcinoma with spindle cell differentiation – Adenosquamous, including mucoepidermoid n Mixed epithelial and mesenchymal – – – Carcinoma with chondroid metaplasia Carcinoma with osseous metaplasia carcinosarcoma
Primary Squamous cell carcinoma <0. 1 % all breast cancer n To diagnose Primary SCC of breast: n – No other breast cancer – Exclude metastases – No skin involvement
Variants of SCC of breast Keratinizing n Spindle cell n Acantholytic n
Clinical presentation n n No specific features Age 31 -83 More in left breast May be fixed to chest wall or extend to skin at presentation Radiology: – No specific findings on mammography – US- cystic lesion.
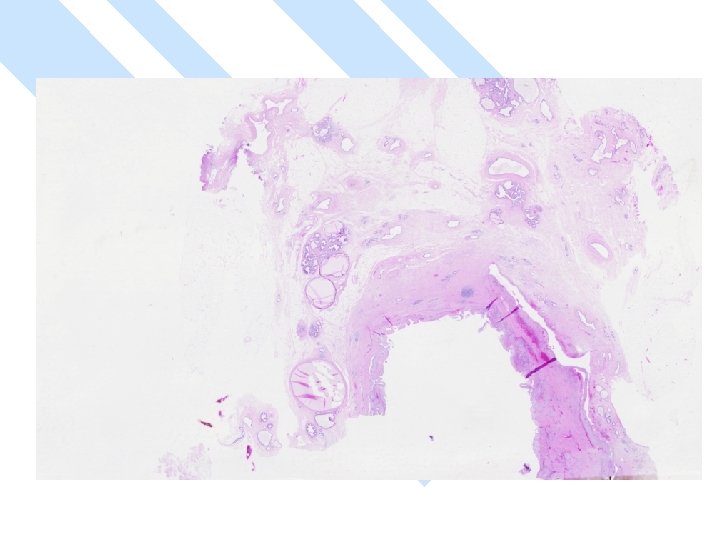
Gross n Size: – vary 1 -10 cm – > 50% > 5 cm – Larger than other types of breast cancer. n Cystic > 50%
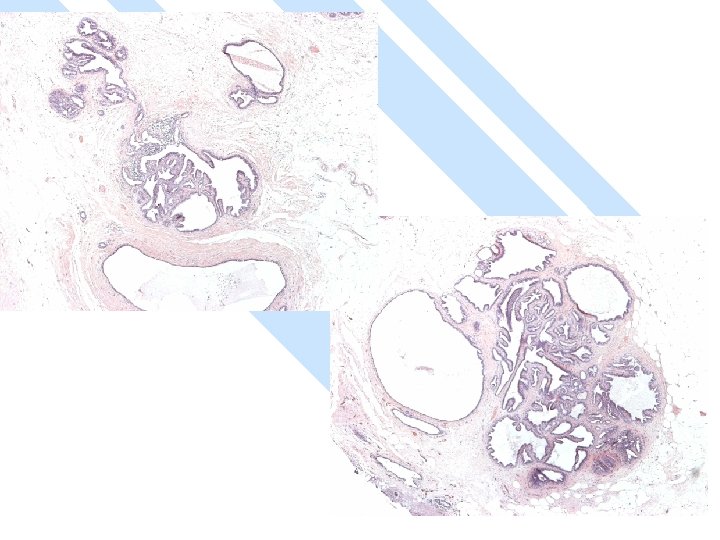
Micro n Exclude metastasis – Most common sites: lung, uterine cervix, urinary bladder. – Cystic degeneration NOT seen in metastatic carcinoma
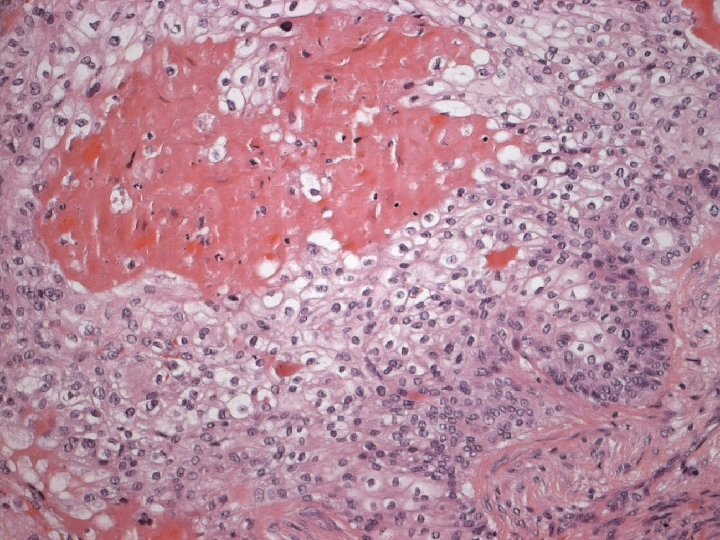
Micro n Similar to SCC at other sites n Cytoplasmic clearing in some
Micro The strongest evidence of a primary SCC of breast is presence of in-situ squamous carcinoma in duct or cyst lining.
pathogenesis Thought to arise from metaplastic squmous epithelium n Reddick proposes that squamous metaplasia arise from myoepithelial cells n Study on squamous metaplasia in a papilloma by IHC & EM.
pathogenesis n Insulin: – enhances development of squamous metaplasia in organ culture of human breast tissue. n Chemical carcinogens: – Keratinising epithelial metaplasia in murine mammary tissue n Estrogen/progesterone effect.
n Squamous metaplasia seen: – Papillomas – Adenomas – Benign phylloides – Benign cysts – Fibroadenomas – Infarcted papilloma/adenoma – Gynecomastia, isolated foci. – Displaced epidermal epithelium by needle core biopsy- epidermal inclusion cyst. – At biopsy sites
n Squamous metaplasia seen: – biopsy sites
n Squamous metaplasia seen: – Lobular hyperplasia
n Squamous metaplasia seen: – Duct hyperplasia
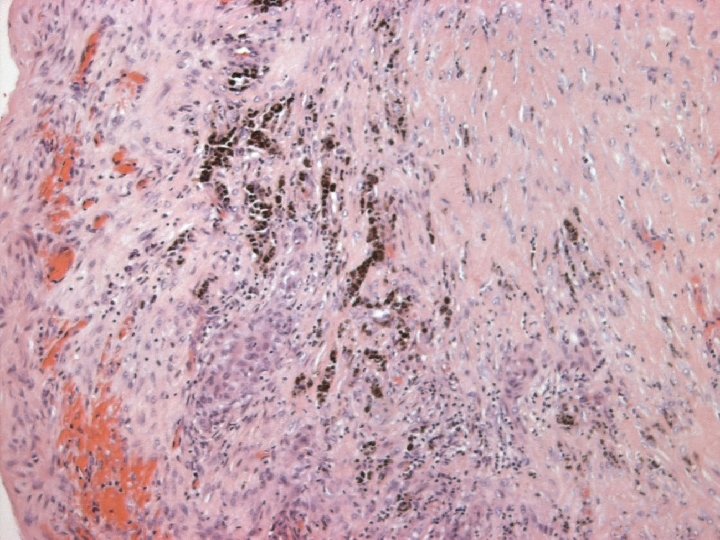
Immunoprofile-SCC n POSITIVE: – Broad spectrum and high molecular weight cytokeratin( CK 5, CK 34ßE 12) n NEGATIVE: – Vascular endothelial markers – ER – PR
Treatment Optimal treatment & prognosis unclear n Stage dependant. Moisidis et al n n Neo-adjuvant chemotherapy & radiotherapy may downstage tumor. Moisidis et al
prognosis n Prognosis : – similar to mammary adenocarcinoma stage for stage. – Poor prognosis for acantholytic subtype – Axillary lymph node metastases UNCOMMON. However rate variable (0 -65%) suggesting a role for axillary lymph node dissection. Moisidis et al n Metastases and local recurrence reported.
Breast lesions & relative risk of subsequent invasive cancer Lesion Nonproliferative breast changes Proliferative breast changes without atypia RR 1 Breast at risk Neither 1. 5 -2 Both breasts Proliferative breast changes with atypia 4 -5 Both breasts Carcinoma in situ 8 -10 Both breasts(LCIS) Ipsilateral(DCIS)
Metaplastic carcinoma “A heterogeneous group of neoplasms characterised by an admixture of adenocarcinoma with dominant areas of spindle cell, squamous, and/or mesenchymal differentiation”
Metaplastic carcinoma n n Represent patterns of gene expression rather than histogenesis. Cell of origin: – Histologic evidence of transition from carcinoma to metaplastic components – IHC studies: » coexpression of S 100, vimentin, CK in both components ( epithelial origin) » Expression of p 63 & p 53 in sarcomatoid components ( origin form myoepithelial cells) n Metaplastic carcinoma: – Heterogenous group of neoplasm that originate from epithelial, myoepithelial or both.
Metaplastic carcinoma n Underreported , ignoring inconspicuous foci. – Fisher et al. reported squamous metaplasia in 3. 7% of invasive carcinoma
Metaplastic carcinoma Age at presentation n Clinical features n Similar to invasive carcinoma • 1 st symptom – palpable mass with rapid growth of short duration • Radiology – not specific except in tumors with osseus metaplasia.
Metaplastic carcinoma n Gross: – Circumscribed contours – Size: 3 -4 cm ( larger than pure infiltrating carcinoma)
Metaplastic carcinoma n Often show focal areas of adenocarcinoma ( ductal) – Require extensive sampling n IHC: – ER/PR negative – vimentin vs. cytokeratin » low & high molecular weight cytokeratin ( express a range of cytoskeletal phenotypes) » CK 5, CAM 5. 2, CK 7 34 BE 12 & AE 1/AE 3. – Mucin n EM
Metaplastic carcinoma n Prognosis: – Rare neoplasm – difficult to identify prognostic factors n n Low frequency of axillary metastases especially in patients with heterlogous elements Axillary lymph node metasteses – 6 -14% squamous and spindle cell metaplastic carcinoma n Disease-free survival at 5 years – 67%
FNA & SCC Cystic tumors yield few if any malignant cells n Show foamy cells seen in cysts of benign fibrocystic changes of breast n
Cysts of breast n Aspiration of cysts When to refer to excisional biopsy – Bloody aspirate – Residual mass – Re-accumulation of fluid – Malignant cytology
References: - - Moisidis et al. Primary squamous cell carcinoma of the breast. ANZ J. Surg. 2002; 72: 65 -67 Roth, Feinberg and Mcavoy. carcinoma arising in the wall of a breast cyst during pregnancy. Ann Surg. Vol. 185. No. 2. 1977 Cibas and Ducatman. Cytology: diagnostic principles and clinical correlates. 2 nd ed. Saunders. 2003. Rosen and Hoda. Breast Pathology: diagnosis by needle core biopsy. 2 nd ed. Lippincott Williams & Wilkins. 2006. Rosen’s breast pathology. 2 nd ed. Lippincott Williams & Wilkins. 2001. - WHO. Pathology and genetics of tumours of the breast and female genital tract. 2003. - Kumar et al. Pathologic Basis of Disease. 7 th ed. 2005. -