ESOPHAGEAL ATRESIA EA WITH TRACHEOESOPHAGEAL FISTULA TEF Esophageal
 WITH TRACHEOESOPHAGEAL FISTULA (TEF).")
 is failure of the esophagus to form a continuous")





 to")



- Slides: 12
ESOPHAGEAL ATRESIA (EA) WITH TRACHEOESOPHAGEAL FISTULA (TEF).
• Esophageal atresia (EA) is failure of the esophagus to form a continuous passage from the pharynx to the stomach during embryonic development. • It is usually associated with TEF. • TEF is an abnormal connection between trachea and esophagus. • Commonly found among premature and LBW babies • Congenital heart diseases or other GI anomalies may present along with these conditions
ETIOLOGY: • Idiopathic • Influencing factors are heritable genetic factor, Teratogenic stimuli, and intrauterine environment. • Failure of the proper separation of embryonic channel into the esophagus and trachea occurs during 4 th and 5 th weeks of gestation.
PATHOPHYSIOLOGY: • Inability to swallow results in accumulation of saliva or feeds in upper esophageal pouch and aspiration in respiratory passage. • Gastric secretions may regurgitate through distal fistula • Abdominal distension occurs due to air entering lower esophagus through the fistula during crying. • Respiratory distress due to gastric distension and elevation of diaphragm.
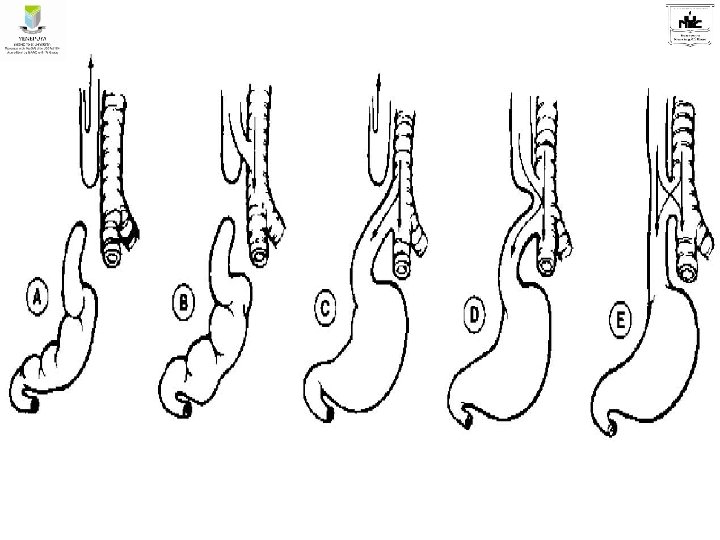
TYPES:
CLINICAL MANIFESTATIONS: • Clinical manifestations appear soon after birth • Baby presents with excessive salivation, constant drooling, large amount of secretions from nose • Coughing, gagging, choking and cyanosis. • On very first feed infant coughs, chokes and fluid returns through nose and mouth. • Infant struggles for breath and cyanosis occurs.
DIAGNOSIS: • Clinical presentation • Inability to pass catheter through nose or mouth into stomach. • Antenatal diagnosis can be done by USG. • Postnatal diagnostic procedures include USG, Plain X-Ray abdomen, Chest X-Ray and passing radio-opaque catheter. • ECG and Echocardiogram to find associated cardiac anomalies
MANAGEMENT: • Immediately after diagnosis infant is kept in propped up position(30 degree) to prevent reflux of gastric secretions, NPO, O 2 therapy, I/V fluid therapy, NG aspiration. • Gastrostomy is done to decompress the stomach and prevent aspiration and later to feed. • Supportive care: nutritional requirement, warmth, prevention of infection, antibiotic therapy, respiratory support, detection and treatment of complications, continuous monitoring of patients, chest physiotherapy and postural drainage.
Surgical Management: • End to end anastamosis with excision of fistula. This is done when the baby is more than 2 Kg and no pneumonia and baby is clinically stable. • Surgical correction is done in stages; Gastrostomy followed by esophageal anastamosis or colonic transplant after one year. This staging is done in very sick and premature babies.
Reference • Hockenberry, Wilson, Judie. Wong’s essentials of pediatric Nursing. South India Edition. Elsevier publication. • Dorothy R Marlow, Barbara A Redding, Raman Kalia. Marlow’s textbook of pediatric Nursing. Harcourt Brace & Company Asia Pte Ltd. • Parul Datta. Pediatric Nursing. 4 th edition. Jaypee Publishers. New Delhi.
THANK YOU