Endometriosis Dr Hima Kandimalla Mount Hope Womens Hospital












































 is commonly")
 • Antiprogestational steroid causes estrogen & progesterone receptors • Dose: 5")















- Slides: 63
Endometriosis Dr. Hima Kandimalla Mount Hope Women’s Hospital Trinidad & Tobago
Endometriosis Presence of endometrial glands & stroma outside the endometrial cavity and uterine musculature
Endometriosis Epidemiology • Globally 90 million suffering with Endometriosis • Prevalence: 3 -10% of reproductive age group & 25 -35% of infertile women • Peak incidence: 30 -45 yrs of age • Prevalence is similar in all races
Endometriosis sites
Endometriosis Pathogenesis Implantation or Metastatic theory - Sampson, 1927 Retrograde menstruation • • More common in young girls with genital outflow obstruction Physiological phenomenon – Halme et al, AJOG, 1984
Endometriosis • Retrograde menstruation ? Contributing factors 1. Alteration in the Endometrium 2. Altered Immune response 3. Favorable Peritoneal environment • Mechanical – Endometriotic foci in surgical scars • Lymphatic or Hematogenous – Extragenital locations
Endometriosis Metaplasia theory – Meyer, 1919 Metaplastic changes in coelomic membrane towards endometrial like tissue following prolonged irritation or Oestrogen stimulation
Endometriosis Genetic, Immunological & environmental factors • 7 times more common in 1°relatives – Halme et al, 1986 & Sampson et al 1980 • More common in Monozygotic twins than in Dizygotic twins – Simpson et al, 1984 • Decreased cellular immunity to endometriotic tissue - Dmowski et al, 1981 • ? Dioxins – Endometriosis association, 1993
Endometriosis Mechanical Endocrine Immunological Implantation Genetic Metaplasia Endometrial implant Progression & invasion Lymphatic & Blood spread Adapted & Modified from – R. W. Shaw, Gynecology
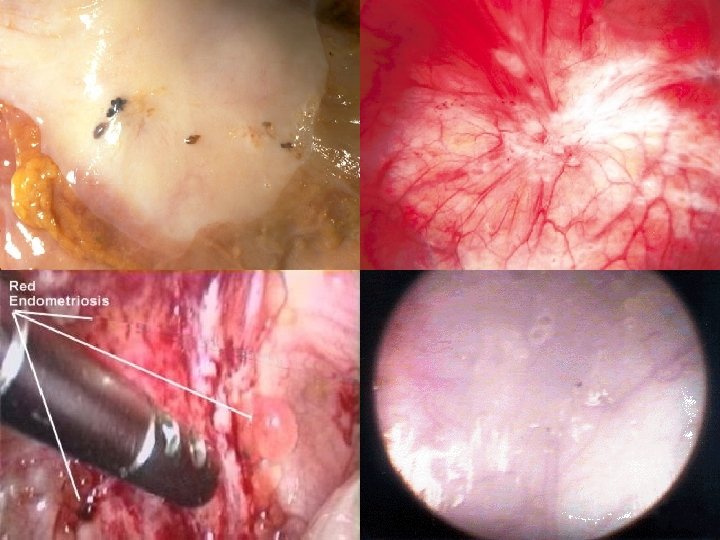
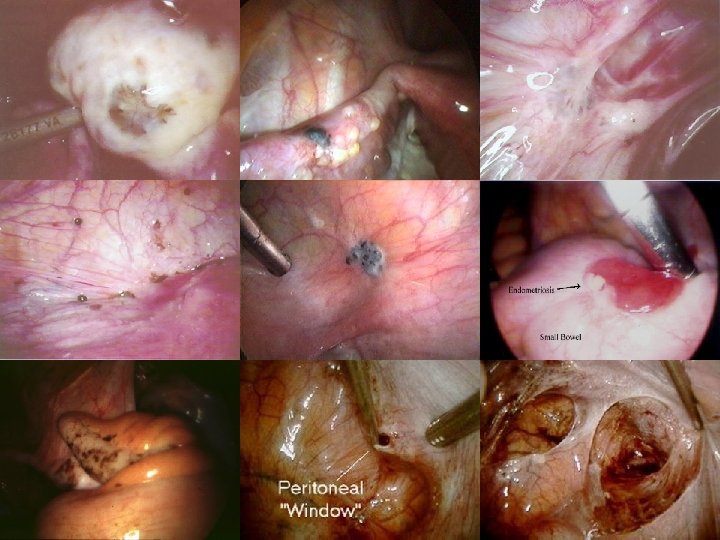
Endometriosis Pathology • Puckered black lesions • White scarring • Red polyps • Clear blebs
White plaques & Clear vesicles Blue-black lesions Newly formed blood vessels
Endometriosis Pathology Endometrioma • Contains blood, fluid & menstrual debris • Brown to black color due to Hemosiderin
Endometriosis Pathology Microscopy • Endometrial glands & stroma • Often contain fibrous tissue, blood & cysts
Endometriosis Stromal endometriosis • Implants contain only stromal component without glandular part • Not hormonal dependent • Locally malignant
Endometriosis Staging – American society of Reproductive Medicine, 1996 Stage I – Minimal Isolated superficial implants, No adhesions Stage II – Mild More superficial implants (<5 cm), No significant adhesions
Endometriosis Staging – American society of Reproductive Medicine, 1996 Stage III – Moderate Multiple superficial & invasive implants, Peritubal & Periovarian adhesions may be present Stage IV – Severe Multiple implants, Ovarian endometriomas, Many dense adhesions
Endometriosis Staging – American society of Reproductive Medicine, 1996 • Staging is designed to predict the likelihood of future fertility • There is no correlation between the stage of disease & the degree of pain or the prognosis with treatment
Endometriosis Diagnosis • Often misdiagnosed • The average time to diagnosis is 9. 28 years – Endometriosis association study, 1998 • Delay in diagnosis: - Progression of symptoms - Infertility till complete reproductive failure
Endometriosis Symptoms Reproductive organs • Dysmenorrhoea • Lower abdominal, pelvic & low back pain • Menstrual irregularities • Infertility
Endometriosis Symptoms GIT • • Cyclical rectal bleeding Tenesmus Dyschesia Diarrhea/ Cyclic constipation • Image courtesy of Dr. Andrew Cook. Visit his site: Endometriosis
Endometriosis Symptoms Urinary tract • Cyclical hematuria • Cyclical dysuria • Ureteric obstruction
Endometriosis Symptoms Lungs • Cyclical hemoptysis • Blood stained Pleural effusions • Catamenial Pneumothorax Haemothorax & ascites associated with endometriosis. - Charran D, Roopnarinesingh S. Department of Obstetrics and Gynaecology, U. W. I. , Trinidad. West Indian Med J. 1993 Mar; 42(1): 40 -1.
Endometriosis Symptoms Umbilicus & Surgical scars • Cyclical pain & swelling
Endometriosis Symptoms • Dysmenorrhoea • Pelvic pain • Infertility • Dyspareunia • Menstrual irregularities • Cyclical dysuria / hematuria • Dyschesia • Cyclic Rectal bleeding 60 -80% 30 -50% 30 -40% 25 -40% 10 -20% 1 -2% <1%
Endometriosis Signs • Pelvic tenderness. • Fixed retroverted uterus. • Nodularity of the Douglas pouch and uterosacral ligaments. • Ovaries may be enlarged and tender. Ovarian cyst may be detected.
Endometriosis Infertility • Clear association with infertility has not been established • Incidence of endometriosis in general population of reproductive age : 2 -10% - Barbieri et al, 1990 • Incidence of endometriosis in infertile women: 20 -40% - Mahmood et al, 1990
Endometriosis Infertility In early stages: • • Activated macrophages in peritoneal fluid PG, IL-1, TNF & proteases in peritoneal fluid levels of anti-endometrial antibodies Luteal phase dysfunction Abnormal follicle growth Multiple premature LH surges LUF syndrome
Endometriosis Infertility In advanced stages: • Pelvic adhesions impairs ova release, blocks sperm entry into the peritoneal cavity & inhibits tubal pickup of the oocyte
Endometriosis Risk of cancer • Ovarian Clear cell & Endometrial cell carcinomas • Breast cancer, Melanoma & NHL - Endometriosis Association study, 1998
Endometriosis Differential diagnosis • Pelvic infection • Uterine Myomas • Ovarian malignant tumors with metastatic deposits in the pouch of Douglas • Acute abdomen • Rectal carcinoma
Endometriosis Investigations Laparoscopy ‘Gold standard’ diagnostic test for endometriosis It permits a “see & treat” approach, although its effectiveness may be limited by the nature of the disease and the surgeon's skill
Endometriosis Investigations Serum CA 125 I 19 II 40 III 77 IV 182 - Cheg YM et al, Obst Gyn, 2002 • Sensitivity 28% & specificity 90% - Mol BW et al, Fertil Steril, 1998 • Not useful for screening, because of poor sensitivity • Can be used to identify a sub-group of women who are likely to benefit from early laparoscopy & to follow the progress of disease after establishing the diagnosis
Endometriosis Investigations Ultrasound Sensitivity for focal endometrial implants is poor
Endometriosis Investigations Ultrasound For Endometriomas sensitivity 83% & specificity 98%
Endometriosis Investigations CT scan • Endometriomas may appear solid, cystic or mixed • Because of poor specificity & high radiation, CT has been replaced by MRI
Endometriosis Investigations MRI • Role is limited in visualizing small endometriotic implants and adhesions • More useful for lesions in extraperitoneal locations & the contents of pelvic mass • More frequently used in staging & treatment response monitoring
Endometriosis Treatment Consider • Age • Symptoms • Stage • Infertility
Endometriosis Treatment Rationale • Recognize Goals: – – Pain Management Preservation / Restoration of Fertility • Discuss with Patient: – – Disease may be Chronic and Not Curable Optimal Treatment Unproven or Nonexistent
Endometriosis Lines of management • • Expectant Medical Hormonal Surgical
Endometriosis Expectant management • Young , asymptomatic infertile patient with mild endometriosis. • If pregnancy does not achieved within 12 - 18 months of observation, hormonal or surgical treatment is indicated.
Endometriosis Medical Treatment Symptomatic pts with minimal or mild lesions • • NSAIDs Opioids.
Endometriosis Hormonal Treatment Produces pseudo pregnancy or pseudo menopause • • • Danazol Progestins Gestrinone Combined oestrogen-progestogen Pills Gn. RH agonists.
Endometriosis Hormonal Treatment Indications • • • Small & superficial lesions Recurrence after conservative surgery Preoperative for 6 -12 wks to decrease size Postoperative for residual lesions When surgery is contraindicated or refused by the patient. Enometriosis in Rectovaginal septum & laparotomy scars doesn’t respond to Hormonal therapy
Endometriosis Danazol • Isoxazole derivative of 17 – alpha ethinyl testosterone • Causes anovulation by • Attenuating the mid cycle surge of LH • Inhibiting multiple enzymes in steroidogenic pathway • Testosterone levels • Dose: 400 – 800 mg/ day for 6 months • Adverse effects: Androgenic effects, effects on serum lipids, Bone mineral density & Liver damage
Endometriosis Progestational drugs • Causes endometrial decidualization & atrophy • Medroxyprogesterone (Provera) is commonly used • Dose: 20 -30 mg/ day for 6 -9 months • Adverse effects: Abnormal uterine bleeding, nausea, breast tenderness, fluid retention & depression
Endometriosis Gestrinone (Ethylnorgestrienone) • Antiprogestational steroid causes estrogen & progesterone receptors • Dose: 5 -10 mg/ wk - dly or twice a wk or 3 times a wk, for 6 -9 months • Adverse effects: deepening of voice, hirsuitism & Clitorial hypertrophy
Endometriosis Combined pills • Well tolerated & can be continued for long term • 1 pill/ day either continuously or cyclically • Continuous regimen is superior in patients with dysmenorrhea • Adverse effects: weight gain, abnormal bleeding & HTN
Endometriosis Gn. RH agonists • FSH & LH & results in endometrial atrophy & amenorrhea • Intranasally or SC or IM with a frequency of twice dly to once in 3 months up to 3 - 6 months • Adverse effects: transient vaginal bleeding, hot flushes, vaginal dryness, libido, breast tenderness, insomnia, depression, irritability, fatigue, headache, osteoporosis, elasticity of skin • Gn. RH agonists + Add-back therapy (estrogens & progestogen) – less side-effects but with same efficacy, can be continued beyond 6 months
Endometriosis Hormonal Treatment The choice between the COCPs, Progestogens, Danazol & Gn. RH agonists depends principally upon their side-effect profiles because they relieve pain associated with endometriosis equally well - Clinical Green Top Guidelines, 2000
Endometriosis Surgical management • Conservative – Excision, Cauterization & Evaporation • Surgeries for pain - Uterosacral Nerve Ablation (LUNA), Presacral Neurectomy • Radical surgeries - Hysterectomy +/- BSO • Surgeries for Endometrioma – Cystectomy, Drainage & coagulation, Fenestration
Endometriosis Surgical management Laparotomy Vs Laparoscopy • • Efficacy is same Laparoscopy – less cost & shorter recovery time even in women with advanced endometriosis
Endometriosis Laparoscopic management 1. 2. 3. 4. 5. 6. Excision Vaporization Fulguration & Desiccation Cystectomy for endomterioma Drainage & Coagulation for endometrioma Fenestration for endometrioma • No RCTs available to compare these procedures • Cystectomy offer better results than drainage & coagulation for Endometrioma • If no cyst wall is present, Fenestration followed by Gn. RH agonists may prove beneficial
Endometriosis Laparoscopic management
Surgical management outcome was poorest in minimal endometriosis • much better in moderate & severe cases • - Sutton CJ et al, Fertil Steril 1994
Endometriosis Combination of Hormonal & Surgical • Postoperative Danazol & Medroxyprogesterone for 6 months lowered the pain scores significantly – Telimaa S et al, Gynecol Endo, 1987 • Postoperative Gn. RH agonist for 6 months lowered the recurrence rates but with no change in pain scores – Parazzini F et al, AJOG, 1994 • Sufficient data is not available to conclude that hormonal & surgical combination is associated with significant benefits. The possible benefits should be weighed in the context of the adverse effects & costs of these therapies - Cochrane review, May 2004
Endometriosis Infertility Management • No role for medical therapy with hormonal drugs • Laparoscopic ablation of minimal – mild endometriosis may improve fertility rates - Cochrane review, 2004
Endometriosis IUI • The presence of endometriosis does not generally impair the results of IUI • Ovarian hyperstimulation using Gonadotrophins with IUI is better than no treatment or IUI alone - Nulsen Jc et al, Obst Gyn, 1993 & Tummon IS et al, Fertil Steril, 1997
Endometriosis Treatment Continue drug therapy Success Pelvic pain & suspected Endometriosis NSAID or OCP Failure Continue Drug therapy Success Empirical Gn. RH agonist + Estro & Prog add-back therapy Failure Operative Laparoscopy Gn. RH agonist + Estro & Prog add-back therapy
Endometriosis Treatment Infertility & Suspected endometriosis Operative Laparoscopy Pregnancy Success Watchful waiting Failure Assisted Reproduction
Endometriosis Conclusion • Endometriosis is a mystery tour as it requires decision making at every stage by the physician and the patient. • Endometriosis still stand as one of the mostinvestigated disorders in gynecology. So is one of the highest priorities for research.
Thank you