DIPHTHERIA Dr Navya N Department of Community Medicine


 Formation- greyish or yellowish membrane(\"false membrane\")- tonsils, pharynx or larynx (or at")






 RESPIRATORY ROUTE- Common. b) NON-RESPIRATORY")




 Early detection : Active search- cases")
 Treatment : (i) CASES : diphtheria-")
 where")







- Slides: 27
DIPHTHERIA Dr Navya N Department of Community Medicine Yenepoya Medical College
INTRODUCTION – Acute infectious disease-toxigenic strains- Corynebacterium diphtheriae. – Three major clinical types : anterior nasal, faucial and laryngeal – Bacilli multiply locally- throat- powerful exotoxin
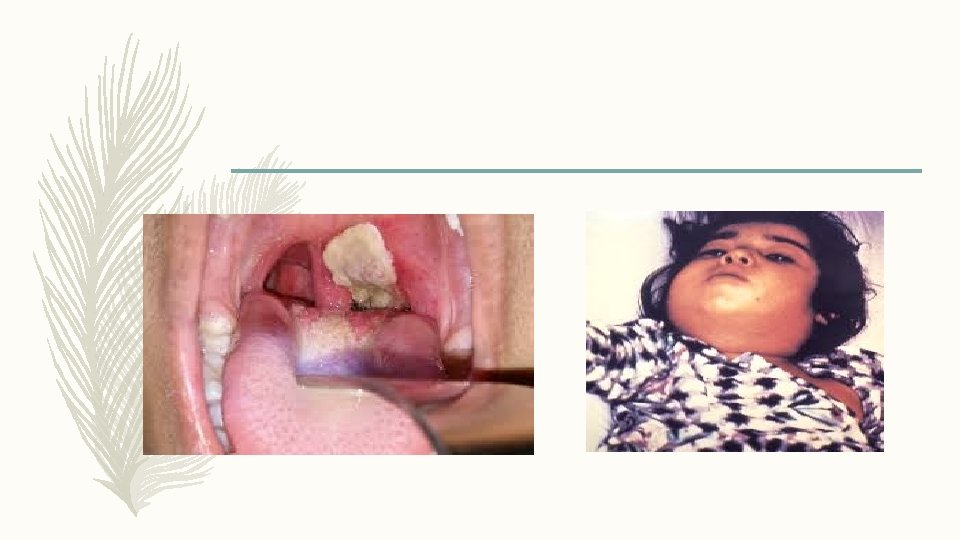
INTRODUCTION (a) Formation- greyish or yellowish membrane("false membrane")- tonsils, pharynx or larynx (or at the site of implantation)- well-defined edges and membrane cannot be wiped away; (b) Marked congestion, oedema or local tissue destruction; (c) Enlargement of the regional lymph nodes; and (d) Signs and symptoms of toxaemia. – Fatality rate- average- 10 % - untreated cases, and 5 % - treated case
PROBLEM STATEMENT WORLD : rare disease –developed countries- routine children vaccination – Improved socio-economic conditions- changing - epidemiology of diphtheria. – Changes- lifestyle - less opportunity to maintain natural immunity- skin infection – Example- waning immunity- outbreak- Russian Federation, Ukraine- 1990 and Thailand Laos in 1996 - highlight- need for booster vaccinations. – Epidemics- largely- decreasing immunization coverage- infants and children, – Developing countries- endemic- lack of adequate widespread immunization – 2012 – 4, 490 cases – globally INDIA: endemic – 2013 – 4090 cases, 64 deaths , case fatality rate – 2. 61
EPIDEMIOLOGICAL DETERMINANTS- Agent Factors – Causative agent : corneybacterium diphtheriae organism. – No invasive power, but produces a powerful exotoxin. – Four types of diphtheria bacilli : gravis, mitis. Belfanti and intermedius- pathogenic to man. – Gravis infections- more severe than mitis. – Not strains- toxigenic. – Non-toxigenic strain- become toxigenic – exposed- particular bacteriophage - carrying the gene- toxin production – Toxin- heart- myocarditis/ nerves- paralysis. – Diphtheria bacilli- sensitive to penicillin and readily killed-heat and chemical agents – Survive for short periods - dust and fomites.
EPIDEMIOLOGICAL DETERMINANTS- Agent Factors – SOURCE OF INFECTION : case or carrier- 0. 1 to 5 per cent 1. CASE- subclinical to frank clinical cases. Mild or silent infection- more important role than frank cases in spreading the infection. 2. CARRIER : ratio- 95 carriers for 5 clinical cases- temporary/ chronic; nasal/ throat – Nasal carriers-particularly dangerous-frequent shedding –organismenvironment, – Temporary- last for about a month; chronic carrier- year or so unless- treated. – lmmunization does not prevent- carrier state.
EPIDEMIOLOGICAL DETERMINANTS- Agent Factors – INFECTIVE MATERIAL : Nasopharyngeal secretions, discharges -skin lesions, contaminated fomites and possibly infected dust. – PERIOD OF INFECTIVITY : Unless treated- 14 to 28 days from- onset- disease. – carriers may remain infective- longer periods. – case or carrier- non-communicable- at least 2 cultures properly obtained from nose and throat- 2 hours apart- negative- diphtheria bacilli
EPIDEMIOLOGICAL DETERMINANTS- Host Factors – AGE : children aged 1 - 5. widespread immunization- shift in age incidencepreschool to schoolage. – SEX : Both sexes are affected, – IMMUNITY : Infants born- immune mothers- relatively immune- first few weeks or months of life. – Developing countries – immunity- inapparent infection. – A herd immunity- over 70% necessary- prevent epidemic – Diphtheria- action- toxin rather than invasion; resistance- availability- specific neutralizing antitoxin - bloodstream and tissues.
EPIDEMIOLOGICAL DETERMINANTSEnvironmental Factors – Occur - all seasons – Winter - months favour its spread MODES OF TRANSMISSION : – Droplet infection. – infected cutaneous lesions. – Transmission by objects (e. g. , cups, thermometers, toys, pencils), contaminated by - nasopharyngeal secretions- possible, but for only short periods.
EPIDEMIOLOGICAL DETERMINANTS- Portal of Entry and Incubation Period a) RESPIRATORY ROUTE- Common. b) NON-RESPIRATORY ROUTES : skin where cuts, wounds and ulcers - not properly attended- may get infected- diphtheria bacilli, – Umbilicus in the newborn. – Occasionally- site of implantation -eye, genitalia or middle ear. – Developed countries – respiratory route- more common INCUBATION PERIOD : - 2 -6 days – occasionally longer
CLINICAL FEATURES – Respiratory tract forms - Pharyngotonsillar, laryngotracheal, nasal, and combinations – Pharyngotonsillar diphtheria- sore throat, difficulty in swallowing, low grade fever – Examination- throat- mild erythema, localized exudate, or a pseudo-membrane. – Membrane- localized/ patch- posterior pharynx or tonsil, may cover entire tonsil, or, cover the soft and hard palates and posterior portion of the pharynx. – Early stage- pseudo-membrane-whitish and may wipe off easily. – Membrane- extend to become thick, blue-white or grey-black, and adherentmucosal erythema- surrounds – membrane – "bullnecked" appearance- severe disease- marked oedema- submandibular area and anterior portion of the neck, along with lymphadenopathy
CLINICAL FEATURES – Laryngotracheal diphtheria- preceded by- pharyngotonsillar disease – Fever, hoarseness and croupy cough at presentation – If infection extends- bronchial tree- most severe form – Initially- clinically indistinguishable- viral croup or epiglottitis. – Prostration and dyspnea- obstruction due to membrane. – Suffocation if not promptly relieved - intubation or tracheostomy
CLINICAL FEATURES – Diphtheria bacilli within- membrane- produce toxin actively. – Toxin – absorbed- distant toxic damage: – parenchymatous degeneration, fatty infiltration and necrosis- heart muscle, liver, kidneys, adrenals, gross hemorrhage – Irregularities- cardiac rhythm- damage- heart. – Difficulties- vision, speech, swallowing. or movement- arms or legs. – Nerve damage- paralysis- soft palate, eye muscles, or extremities – Patients- survive- complications recover completely.
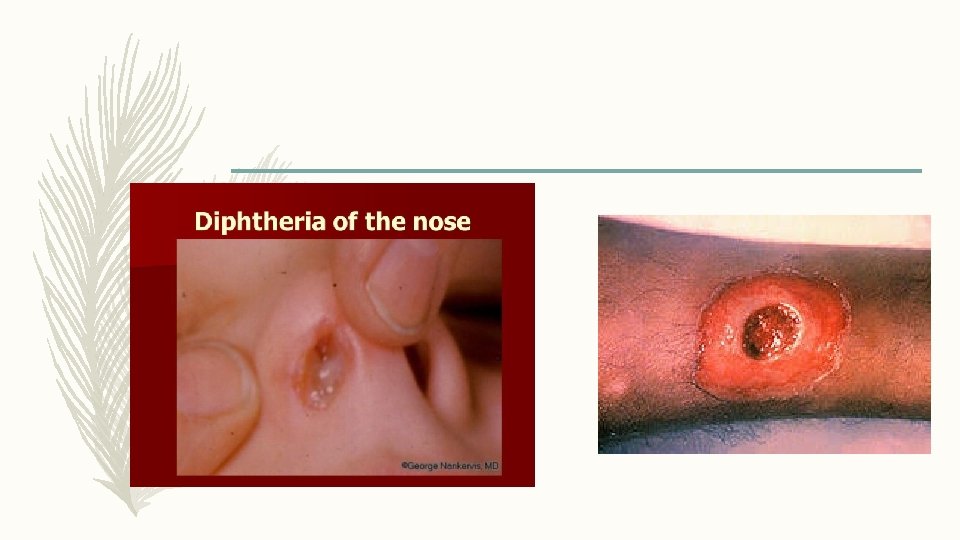
CLINICAL FEATURES – Nasal diphtheria – mildest form of respiratory diphtheria- localized- septum/ turbinates – Occasionally- membrane- extend into - pharynx – Non-respiratory mucosal surface- conjunctivae and genitals may also- sites of infection. – Cutaneous diphtheria- common- tropical areas- appears- secondary infectionprevious skin abrasion/ infection. – Presenting lesion- an ulcer- surrounded by erythema and covered with a membrane. – Patients- seek treatment- chronicity of skin lesion.
CONTROL OF DIPHTHERIA – CASES AND CARRIERS (a) Early detection : Active search- cases and carriers- start immediately- family and school contacts. – Carriers- detected only- culture method. – Swabs- taken- both nose and throat and examined- culture methods (b) Isolation : All cases, suspected cases and carriers- promptly isolated – preferably- hospital- at least 14 days or until proved free of infection. – At least 2 consecutive nose and throat swabs- 24 hours apart-negative before terminating isolation.
CONTROL OF DIPHTHERIA – CASES AND CARRIERS (c) Treatment : (i) CASES : diphtheria- suspected- antitoxins- given without delay- IM/ IV – Dose- 20, 000 to 100, 000 units or more- upon- severity- case , after- preliminary test dose- 0. 2 ml subcutaneously – Mild early pharyngeal or laryngeal disease- 20, 000 -40, 000 units; – Moderate nasopharyngeal disease- 40, 000 -60, 000 units – Severe, extensive or late (3 days or more) disease, 80, 000 -100, 000 units – Every case- Antitoxin + penicillin or erythromycin- 5 to 6 days – (ii) CARRIERS : 10 day course- oral erythromycin- most effective drug – treatment of carriers.
CONTROL OF DIPHTHERIA – CONTACTS: special attention- throat swabbed- immunity status determined. (a) where primary immunization or booster dose- received within - previous 2 years, no further action- needed (b) where primary course or booster dose- diphtheria toxoid- received more than 2 years before, only- booster dose- diphtheria toxoid (c) non-immunized close contact- prophylactic penicillin or erythromycin. – 1000 -2000 units- diphtheria antitoxin and actively immunized against diphtheria. – Contacts- medical surveillance and examined daily - atleast a week after exposure – Bacteriological surveillance- close contacts- several weeks- repeated swabbingapproximately weekly intervals
CONTROL OF DIPHTHERIA – COMMUNITY – Only effective control- active immunization- diphtheria toxoid- all infants as early in life as possible, as scheduled. – Subsequent booster doses every 10 years thereafter – Aim- immunize before- infant loses- maternally derived immunity – Vaccine- toxoid- not directed against organisms- does not prevent- carrier state – Nonimmune individuals- not protected- high level - population immunity – Immunization rate- maintained at a high level
DIPHTHERIA IMMUNIZATION a. Combined or mixed uaccines : b. Single Vaccines : – DPT (diphtheria-pertussis-tetanus vaccine) – – DTPw (diphtheria, tetanus, wholecell pertussis) – PTAP (purified toxoid aluminium phosphate) – DTPa (diphtheria, tetanus, acellular pertussis) – DT (diphtheria-tetanus toxoid) – d. T (diphtheria-tetanus, adult type) FT (formal-toxoid) – APT (alum-precipitated toxoid) – PTAH (purified toxoid aluminium hydroxide) – TAF (toxoid-antitoxin floccules) c. Antisera- Diphtheria anti-toxin.
COMBINED VACCINES – Immunizing infants- preparation of choice- DPT. – infant can be immunized simultaneously against three diseases- great gain administratively. – Pertussis component- enhances- potency- diphtheria toxoid. – Two types- DPT vaccine - plain and adsorbed. – WHO recommends- only adjuvant DPT preparations- utilized- immunization programmes
COMBINED VACCINES – PENTAVALENT VACCINE – Dose – 0. 5 ml – Number of doses – 3 – 6, 10 and 14 weeks – Route of administration- Intramuscular (IM) – Site – Anterolateral side of mid thigh ( left ) – Maximum age – till 1 year – Booster 1 - 16 -24 months – DPT – IM 0. 5 ml- Anterolateral side of mid thigh (left) – Booster 2 – 5 -6 years – DPT - IM 0. 5 ml- Left Upper arm – For children over 12 years – d. T – adult type diphtheria tetanus vaccine – 2 doses – 4 -6 weeks apart, booster – 6 -12 months after 2 nd dose
COMBINED VACCINES REACTIONS AND CONTRAINDICATIONS – Fever and mild local reactions – common – Severe complications- Pertussis component - neurological- encephalitis/ encephalopathy ) - prolonged convulsions - infantile spasms - Reye’s Syndrome CONTRAINDICATIONS : – Previous – severe reaction – DPT not repeated instead DT given
SINGLE VACCINE AND ANTISERA – Single vaccines less frequently used ANTISERA : – Diphtheria antitoxin – horse serum – mainstay of passive prophylaxis – Protection against diphtheria toxin – quantitative phenomenon
SUMMARY – Acute infectious disease-toxigenic strains- Corynebacterium diphtheriae. – Three major clinical types : anterior nasal, faucial and laryngeal – Mode of spread – respiratory and non respiratory – Bacilli multiply locally- throat- powerful exotoxin – Formation of greyish membrane ( false membrane ) – Bull necked appearance – Pentavalent vaccine