CORYNEBACTERIUM DIPHTHERIAE Hippocrates provided the first clinical description

CORYNEBACTERIUM DIPHTHERIAE

Hippocrates provided the first clinical description of diphtheria in the 4 th century B. C. Bretonneu (1821), a French army surgeon, described the unique clinical characteristics of the disease, and used the term ‘dipht`erie’ to signify the tough leathery pseudomembrane that occurs in oropharynx and some times in nasopharynx. (diphtheros = leather)

First described by Klebs in 1883. Cultivated by Loeffler in 1884, identified Corynebacterium diphtheriae as the agent of the disease. In 1884, Loeffler concluded that C. Diphtheriae produced a soluble toxin, and provided the first description of a bacterial exotoxin. Roux and Yersin (1888) discovered the diphtheria exotoxin and established its pathogenic effects. The antitoxin was described by von Behring (1890)

The Corynebacteria Genus: Corynebacterium. Gram positive, Non-sporing, Non motile bacilli. Arranged in Chinese letter pattern Or Cuneiform pattern. Characteristic club shaped appearance due to irregular swelling at one or both ends. Hence the name “Corynebacterium” Club in Greek.

Classification C. diphtheriae – Most important pathogen, causing the childhood disease, Diphtheria. Mc. Leod and Anderson classified diphtheria Based on the colony characteristics on Tellurite medium and biochemical reactions and severity of disease; • Biotypes – gravis – intermedius – mitis – belfanti

C. ulcerans – acute pharyngitis with lesions clinically resembling diphtheria. C. xerosis – conjunctival sac. C. pseudodiphtheriticum – throat
 ü Resemble C. diphtheriae. ü Occur as commensals in")
v Diphtheroids (Non diphtheria Corynebacterium) ü Resemble C. diphtheriae. ü Occur as commensals in the throat, conjunctiva and urinary tract. ü In immunocompromised patients they may cause Pneumonia, Infective Endocarditis, Shunt or Canula infection, Soft tissue / Bone / Cutaneous infection.

Corynebacterium diphtheriae Most important member of the genus and is the causative agent of the dreaded childhood disease – Diphtheria. Bacterial Virulence factors -> The pathogenic effect of C. diphtheriae is due to the production of a powerful exotoxin – Diphtheria toxin

Diphtheria toxin Ø A potent exotoxin produced by toxigenic strains of C. diphtheriae. symbiotic bacteriophage Tox β phage (gene coding for toxin production) Non toxigenic strain Toxigenic strain Lysogenic conversion

Properties of Diphtheria toxin -> 1. Potent exotoxin (Lethal at 0. 1 µg/kg body weight). 2. Polypeptide (MW 62, 000). 3. Heat labile 4. Highly antigenic. 5. Antibodies (antiserum) are protective. 6. Has cytotoxic, cardio-toxic and neurotoxic activities.

Structure - Made up of 2 subunits. ü A - Active unit: responsible for the toxic action. ü B - Binding unit: helps in binding to target cell & in translocation of subunit A into cell. Mode of action Ø Inhibition of protein synthesis. Leads to cell death (cytotoxic action).
’ from NAD+. ADPR")
“ADPR-EF 2” Catalyses the transfer of ‘adenosine complex diphosphate ribose (ADPR)’ from NAD+. ADPR binds with the elongation factor EF 2. Protein synthesis stops abruptly

Pathogenesis and clinical features Source of infection -> Ø Humans –> - Carriers ( most important) - patients Organisms are found in the respiratory tract or wounds. Mode of transmission -> Ø Inhalation of respiratory droplets Ø Contact with the contaminated articles (fomites)

Sequence of events -> Entry of the virulent organisms into a susceptible individual by inhalation Attachment to the mucus membrane of the upper respiratory tract Colonization, multiplication & toxin production Toxin absorbed by the host, resulting in - Local inflammation - Distant toxic damage of tissues & organs Symptoms of diphtheria

Diphtheria Ø The bacilli remain confined to the site of entry, where they produce toxin. Ø The toxin causes local necrotic changes -> pseudomembrane formation, which is characteristic of diphtheria infection. Ø The mechanical complications of diphtheria are due to membrane, while systemic effects are due to toxin.

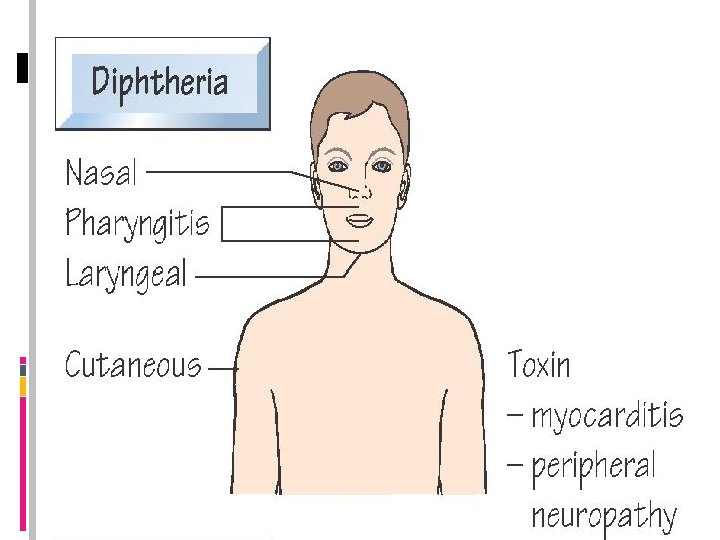
Incubation period - 2 – 6 days Clinical features of Diphtheria 1. Based on site of infection -> Diphtheria is classified as - Faucial - Laryngeal - Nasal - Otitic - Cutaneous

2. Based on severity of disease -> Ø Hypertoxic –> severe toxaemia with marked adenitis (bull neck) is observed. Ø Hemorrhagic - hemorrhage at the edges of pseudomembrane Generalized bleeding tendency. Ø Septic -> ulceration, cellulitis, sepsis.

Clinical features Diphtheria toxin is absorbed into the mucus membrane and causes destruction of epithelium and a superficial inflammatory response Local effects. Fever, Sore throat, Cervical Adenitis and Pseudo membrane formation over the Tonsil and Throat Bacilli produce more toxin -> absorbed into the systemics causing Distant toxic damage

A. Local effects -> 1. Pseudomembrane -> Ø A thick, bleeding, greyish, adherent, pseudomembrane consisting of necrotic epithelia, exuding fibrin, RBC’s, WBC’s and the organisms is formed, commonly over the tonsils and throat.

2. Marked cervical adenitis & lymphadenopathy results in edema of the entire neck region resembling a - bull neck

B. Distant toxic effect / damage Ø Parenchymatous degeneration Ø Fatty infiltration Ø Necrosis of Heart muscle, Liver, Kidneys & Adrenals. Gross hemorrhage Neurotoxicity -> paralysis of soft palate, eye muscles & extremities

Complications -> 1. Obstructive complication due to pseudomembrane – Ø When pseudomembrane extends into larynx and trachea it can cause airway obstruction thereby leading to death from asphyxia. Ø Emergency intubation or tracheostomy is indicated.

2. Acute circulatory failure and shock – Ø due to cardiotoxic effect of diphtheria toxin. 3. Post diphtheria paralysis Ø due to neurotoxic effect of toxin. Ø occurs 3 - 4 weeks after appearance of diphtheria. Ø Symptoms slowly subside spontaneously.

Cutaneous diphtheria May occur when C. diphtheriae infects open wounds. Ø Ulcerating skin lesion covered by a grey membrane that fails to heal is seen. Ø Systemic effects are negligible.

Types / Symptoms of Diphtheria

Laboratory diagnosis

This is to confirm the clinical impression and for epidemiological purpose; Specific treatment must never be delayed for laboratory reports, if the clinical picture is strongly suggestive of diphtheria; Any delay may be fatal…!

Laboratory diagnosis consists of Isolation of the organism and demonstration of it’s toxicity; Methods include Microscopy. Culture. Demonstration of toxigenicity. Specimens : Swabs from – Nose, Throat or other suspected lesions

If the swabs can not be inoculated promptly, they should be kept moistened with serum; Inoculate on : – Loeffler’s serum slope – Tellurite blood agar or Tinsdale medium – Blood agar ( for differentiating Staphylococcal or Streptococcal pharyngitis that simulate diphtheria); Tellurite medium is particulary useful for isolating the organism from – convalescents, contacts or carriers;

Microscopy Gram stained smear Ø Slender, Gram positive , Pleomorphic bacilli. Ø which posses irregular swelling at one or both ends give them a club- shaped appearance.

Metachromatic granules –They are often situated at poles- ‘polar bodies’ ü Also known as ‘Volutin granules’ ; ‘Babes-Ernst’ granules. ü Chemical nature – polymetaphosphate. ü Function – Nutrition or energy reserve. ü Demonstrated by – Albert’s staining method. ü May also be present in – diphtheroids / Lactobacilli / Bacteroides / Pseudomonas

Albert’s staining method Ø Green bacilli with bluish black granules Ø Bacilli are arranged in a characteristic “Chinese letter pattern”.

Neisser’s stain: Cytoplasm appears light brown. Granules blue black Ponders stain : weak solution of toludin blue.

Culture Media Blood agar - Non-selective enriched medium. Loeffler’s serum slope - Enriched medium. Ø C. diphtheriae grows at a faster rate than other organisms & therefore may be separated from other oral flora after incubation for 6 hrs. Ø Metachromatic granules are better formed when grown on this medium.

Cystine Tellurite blood agar - Selective medium Ø Tellurite inhibits oral flora. Ø C. diphtheriae grows slowly (36 - 48 hrs). Reduces tellurite to metallic tellurium -> Brown to black with a brownblack halo
: – Grey black colonies")
Tinsdale’s medium (also contain cystine in addition to tellurite): – Grey black colonies with dark brown haloes indicate C. diphtheriae and C. ulcerans.

Incubation Ø Media are incubated at 370 C, aerobically for up to 72 hrs. Identification of isolate - Loeffler’s serum slope Blood Agar Tellurite blood Agar Moist colonies Hemolytic / Black colonies on by 6 hrs Non Hemolytic colonies

ü Albert’s staining: Smears from the colonies will show typical bacilli with metachromatic granules. ü Sugar fermentation: Using Hiss serum sugars – C. diphtheriae ferments with acid production, glucose, galactose, maltose but not lactose. ü Urease test : Negative All isolates identified as C. diphtheriae should be tested for toxin production.

Toxigenicity testing Ø To detect whether C. diphtheriae isolated from a patient can produce toxin. In - vivo methods Using Guinea pigs or Rabbits - Subcutaneous test - Intradermal (intracutaneous) test In - vitro methods - Elek’s gel precipitation test - Tissue culture test

SUBCUTANEOUS TEST Emulsify the growth form an overnight culture of Loeffler’s serum slope in 24 ml broth 0. 8 ml injected subcutaneously Into two guinea pigs Control animal Protected with 500 IU of Antitoxin 18 -24 hrs previously Remain healthy Disadvantage : Death of the animal Test animal Unprotected Die in 4 days if the strain is Virulent; autopsy shows Characteristic features

INTRACUTANEOUS TEST 0. 1 ml of emulsion broth inoculated intracutaneously in to two guinea pigs Test animal Control animal Should receive 500 IU Of antitoxin previous day Give 50 IU of antitoxin Intraperitoneally 4 hrs after skin test (To prevent death) NO CHANGE Inflammatory reaction Progress to necrosis in 48 -72 hrs Animal does not die; Rabbits may also be used; As many as 10 strains can be tested simultaneously;

Elek’s Gel Precipitation Test 20% horse serum agar. Arrow head precipitation band indicates toxin production incubated at 370 C for 24 -48 hours paper strip saturated with 1000 units of diphtheria antitoxin Test organism Controls

Tissue culture test – Ø A petri dish monolayer cell culture with agar overlay is used. Ø Test organism is inoculated. Ø If isolate is toxigenic the toxin diffuses into cells below and kills the cells.

Treatment 1. Neutralization of absorbed toxin -> ü Most important step, should be carried out immediately in clinically suspected diphtheria. ü Specific Antitoxin - Anti diphtheria serum (ADS) raised in horses. ü 20, 000 – 100, 000 units of antitoxin are injected IV or IM. (Precautions to rule out hypersensitivity to animal protein)

2. Antibiotic treatment ü Has no effect on toxin already absorbed into the systemics. ü Helps in elimination of organism; thereby preventing further toxin production. ü Penicillin / Erythromycin – Drug of choice

Prevention Aim of prevention – ü To maintain a high level of active immunization. By active immunization of the target population - children ü To limit spread of toxigenic diphtheria bacilli in a population. Isolation of patients. Early treatment.

Active immunisation Emil von Behring initiated immunisation in children in 1913 using toxin –antitoxin mixtures; (TAT). These preparations were hazardous. • In 1929, Ramon introduced ‘toxoid

Active immunization Triple Antigen Vaccine – DPT Contains Toxoids : C. diphtheriae and Cl. Tetani. killed suspension(whole cell): Bordetella pertusis. Provides protection against Diphtheria Pertusis Tetanus.

Composition 0. 5 dose if formulated to contain Diphtheria toxoid: 6. 7 -12. 5 Lf units Tetanus toxoid : 5 Lf units Pertusis vaccine: ≤ 16 opacity units

Ø Recommended schedule for active immunization of children with DPT – Ø IM or SC route ü 1 st dose – 6 to 8 weeks ü 2 nd dose – 10 to 12 weeks ü 3 rd dose – 14 to 16 week ü 1 st Booster – 18 th month ü 2 nd Booster – 5 th year

Side effects. Usually because of pertusis component 20% of children mild side effects such as Local inflammation and Fever. About 0. 1% experience convulsions. 1 in 150, 000 experience severe or irreversible brain damage. Ø It is advisable not to carry out routine immunization if poliomyelitis is active in the area because of possibility of prvocative poliomyelitis.

Alternatives: DTa. P Contains acellular pertusis vaccine with combination of diptheria and tetanus toxoids. DTa. P/Hib In addition it contains vaccine against haemophilus influenzae type b(Hib).

Combined Immunization To all children in a pediatric ward when a diphtheria case is admitted Passive immunization - 500 - 1000 units of ADS (Antidiphtheritic serum ) on one arm Active immunization - 1 st dose of DT on other arm If there is no history of vaccination, active immunization course is completed 2 nd dose -> after 2 months; 3 rd dose -> 6 – 12 months later

THANKS
- Slides: 55