Definition of FESTINATING GAIT HOEHN AND YAHR CLASSIFICATION
















Repetitive Slow Rhythmical Vestibular Stimulation Eg – Rocking Chair")
 Deep Breathing Exercises 4) Stress Management A Daily Schedule has to be Planned")






 Combination of UL & Trunk Movements and Perform")


Clothing 2)Lying to Sitting 3)Sit to Stand 4)Gait ADAPTATION -Loose Fitting Clothes With")

Weight Transference, Pelvic & Trunk Movts 2) Increase Stride Length & Base of")

- Slides: 37
Definition of FESTINATING GAIT HOEHN AND YAHR CLASSIFICATION OF DISABILITY DIAGNOSIS Medical Management Physical Therapy Management
Parkinson’s Disease is a chronic progressive degenerative disease of the nervous system. § Patient typically exhibit classic clinical signs of Rigidity, Bradykinesia, Resting. Tremor and Impaired Postural Reflexes.
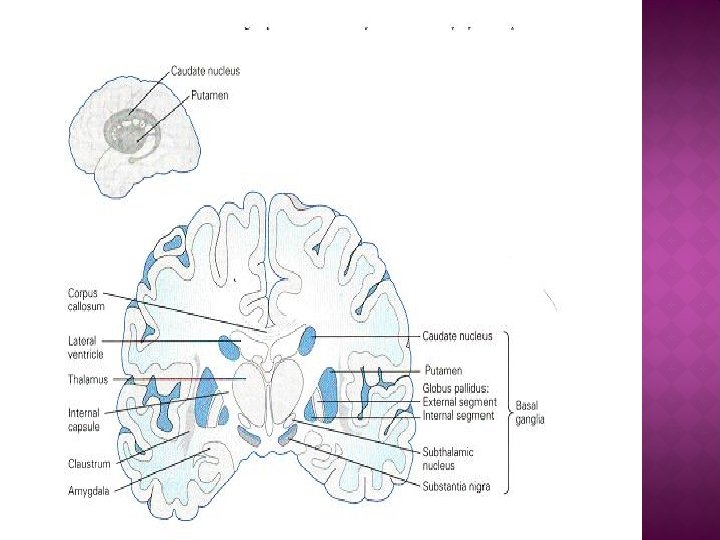
The Basal ganglia are a group of nuclei located at the base of the cerebral cortex. The three main nuclei of the basal ganglia include the Caudate, Putamen, and the globus pallidus. The other subcortical nuclei are Subthalamic nuclei and Substantia Nigra.
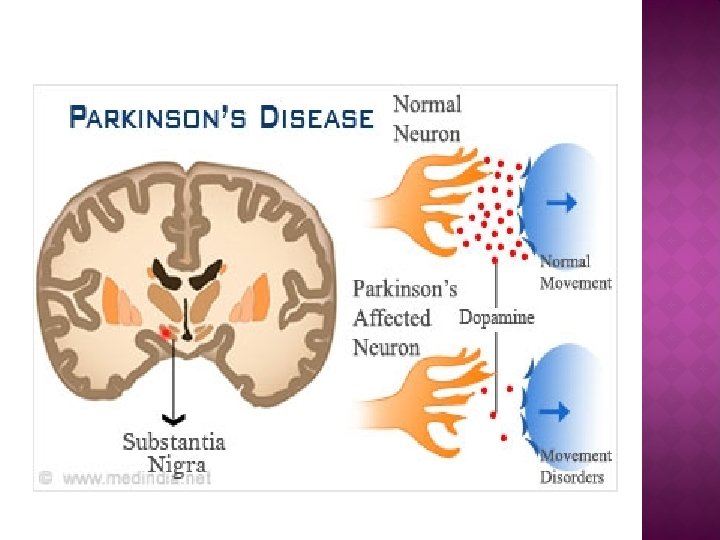
�The Substantia Niagra contains Neurons which produces Dopamine. �The Caudate Nucleus contains Neurons that produce Ach. �In PD there is degeneration of Dopamine producing neurons in Substantia Niagra. �So there is Decrease in Dopamine (Inhibitory) �The normal Cholinergic pathways (Excitatory) overacts and leads to imbalance and exhibits the sign of parkinsonism
RIGIDITY Rigidity is defined as Resistance to Passive motion that is not Velocity Dependent. Rigidity may initially affect one side and eventually spreads to involve the whole body. BRADYKINESIA It refers to Slowness and difficulty in maintaining movements.
TREMOR An Involuntary Oscillation of a Body part occurring at a slow Frequency of 4 -7 / Sec The Parkinsons Tremor is described as RESTING TREMOR It typically presents at Rest and Disappears with Voluntary Movement. PILL ROLLING TREMOR � Opposition of Index and Thumb. � Resting Tremors may also seen in Feet, Lips, Tongue & Jaws.
POSTURAL INSTABILITY Frequent Falls results due to Progressive loss of Balance Reactions. Postural Reactions becomes Increasingly impaired as the disease progresses.
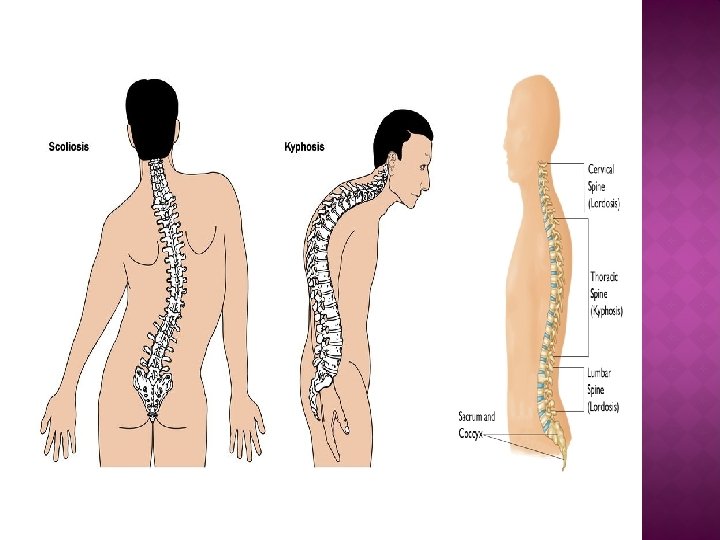
POSTURAL GRADING 1. Normal 2. Head Protruding 3. Head Protruding with Marked Kyphotic Thoracic Spine, Slight Flexion at Knees & Elbows. 4. Marked Flexion of Trunk, Elbows, Hips & Knees.
Fatigue Edema – In Feet & Ankle Masked Face Postural Deformities – Kyphosis, Scoliosis Osteoporosis Swallowing Difficulties Micrographia – Abnormally small hand writing Visual Abnormalities Sensory disturbances
Abnormally small hand writing seen in Parkinson’s Disease
FESTINATING GAIT Due to Abnormal Stoop Posture, Gait is characterized by a progressive increase in Speed & Shortening of the Step The Patient takes Multiple Short Steps to catch up the Centre of the Mass & Avoid Falling And Eventually break into a Run Turning & Changing Directions are difficult
STAGE 1 2 3 4 5 CHARACTER OF DISABILITY Minimal or Absent; Unilateral if present Minimal Bilateral or Midline involvement Balance not Impaired Righting Reflexes, Unsteadiness When turning or rising from chair. Some activities are restricted, but patient can live Independently and continue some form of Employment. All symptoms are present and severe. Standing and walking possible only with Assistance. Confined to bed or Wheelchair.
§ § § A Diagnosis can be made if At least 2 of the 4 Cardinal Features are Present Hand Writing Samples, Speech & Physical Examinations are Performed Glabellar reflex It is elicited by repetitive tapping on the forehead. Subjects blink in response to the first several taps. If the blinking persists, this is known as Myerson's sign – seen in Parkinson’s disease. Myerson's sign
§ Atrophy of Substantia Niagra is noted. § Mostly Help Full in Ruling Out Other CNS Pathologies
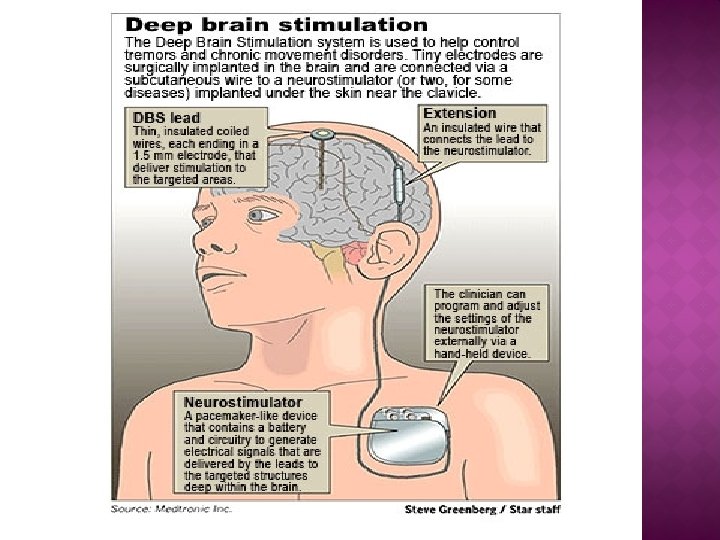
MEDICAL MANAGEMENT ANTICHOLINERGIC DRUGS Trihexyphenidyl Bentropin DOPAMINERGIC DRUGS Levadopa Carbidopa Sinemet SURGICAL MANAGEMENT § § § Pallidotomy -the surgeon destroys a tiny part of the globus pallidus Thalamotomy Deep Brain stimulation-is a neurosurgical procedure involving
§ § § § Relaxation exercises ROM exercises & Stretching Facial exercises Respiratory Management Balance training Aerobic exercises Functional mobility exercises Gait training
Relaxation can be achieved by 1)Repetitive Slow Rhythmical Vestibular Stimulation Eg – Rocking Chair 2)Slow Rhythmic Rotations in Small Range Activities Supine Lying Side To Side Head Rotation Upper Trunk Rotation PNF Patterns- Shoulder – D 2 - Flexion (Flx, Abd, ER) D 2 - Extn ( Ext, Add, IR) Hook Lying – Lower Trunk Rotations
3) Deep Breathing Exercises 4) Stress Management A Daily Schedule has to be Planned Time Management for each Activity Since He has Planned in Advance, He can manage to Perform the Activities without Anxiety & Stress, This Promotes Relaxation
Active ROM Exercises are Performed 2 -3 times Daily If Active ROM is Difficult Active Assisted or Passive Rom can be done Exercises should Focus on Strengthening Patient `s Weak Elongated Extensor Muscles and Stretch the Tight Flexor Muscles
STRETCHING Stretching can be done by means of PNF Techniques like Hold Relax or Traditional Stretching Techniques In Traditional Stretching, Slow Sustained Stretch for 30 sec is performed 3 to 5 times
FACIAL EXERCISES Facial Movements such as Frowning, Smiling, Lip Pursing Movements of the Tongue Opening & Closing of the Mouth Visual Feedback – Mirror
RESPIRATORY MANAGEMENT The Management Includes Deep Diaphragmatic Breathing Exercises Segmental Breathing Exercises Breath Control Techniques ( Insp : Expr – 2 : 3) Neck, Shoulder & Trunk Mobility Exercises Improving Postural Awareness & Correction by Visual Feedback (Mirror)
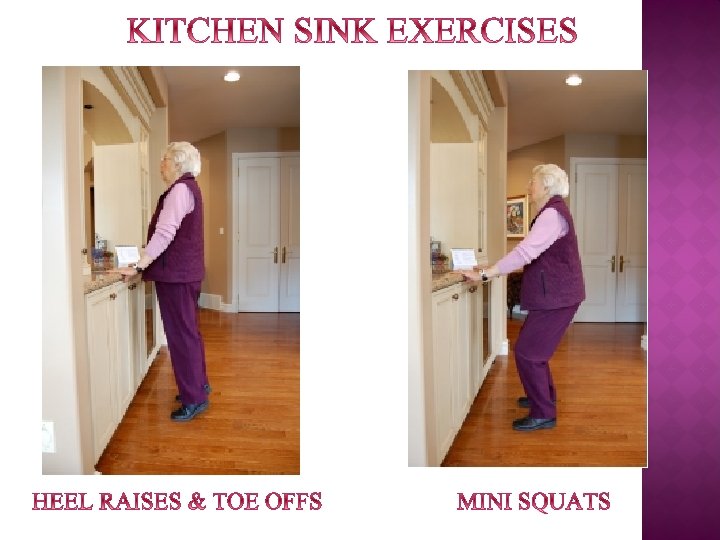
BALANCE TRAINING ü Sitting balance ü Sit to stand transition ü Standing balance ü Kitchen sink exercises SITTING BALANCE Weight Shifting Techniques combined with UL Movements (Reach) in all Directions This promotes Trunk Movements in All Directions Swiss Ball can also be used to train Balance
BALANCE TRAINING SIT TO STAND TRANSITION From High Seated Chair & Progression by Reducing the Height of the Chair Assistance can be given in the form of Physical Support by the Therapist or Patient Himself holding a Wall Bar during Transition STANDING BALANCE Adequate Strength & ROM are Important components needed to Withstand the challenges of Balance
BALANCE TRAINING Activities in Standing 1) Combination of UL & Trunk Movements and Perform Reach in all Directions 2) Perturbations in all Directions
Cardiopulmonary Endurance can be Improved by Participating in Regular Aerobic Conditioning Program. Mode Walking Bicycle & Arm Ergometer Intensity Sub maximal Frequency & Duration According to the Individual's Ability Group Training is more beneficial Starting with warm- up, Activity & followed by
ACTIVITY 1)Clothing 2)Lying to Sitting 3)Sit to Stand 4)Gait ADAPTATION -Loose Fitting Clothes With Velcro Closures - Monkey Rope - Firm Chair With Arm Rest - Cane for Assistance
SPINAL MOBILITY EXERCISES Extension Activities Prone on Elbows & Prone on Hands Promotes Spinal Extension Standing Wall Push Ups Side Flexion & Rotation Transition from Side Lying to Sitting Promotes Side Flexion & Rotation of the Trunk
Goals 1)Weight Transference, Pelvic & Trunk Movts 2) Increase Stride Length & Base of Support 3) Reciprocal Arm Swing 4) Rhythm 5) To Promote Normal Heel Toe Progression Activities - Static Marching, Stepping Forward & Backward & wt Bearing - Floor Markings ( Visual – Cues) - Wand - Oral Counts ( Auditory - Cues) - A Wedge is placed inside the shoe
OTHER ACTIVITIES Starting & Stopping Walking Sideways Walking Across Obstacles Turning Around Regular Walking Exercises to Prolong Functional Independence