Childhood cough A forced expulsive manoeuvre against a





 Feature Diagnosis • Snotty • Barking cough • Tachypnoea,")



")

 • • • Grey area Still likely viral")











 • Conducting airways disease – a")




- Slides: 33
Childhood cough A forced expulsive manoeuvre against a closed glottis by a child Dr Steve Wadams Consultant Paediatrician steve. wadams@poole. nhs. uk
Aim to cover • • • Acute vs Chronic cough Targeted history and examination Red flags in red Investigations/referral/treatment Old, new and recycled thoughts on cough Occasional personal practice points in red italics
Why concentrate on cough? • Common reported • Annoying • Anxiety provoking • Lots of remedies on sale • Wide differential of causes • BTS guidance in 2008 by whom? to whom? in whom? Why?
Cough timelines • Often difficult to establish start • Recurrent (>2 episodes, unrelated to URTI in a year) • Acute <3 weeks, prolonged 3 -8 weeks and chronic >8 weeks I often draw disease progression with parents
An acute cough timeline
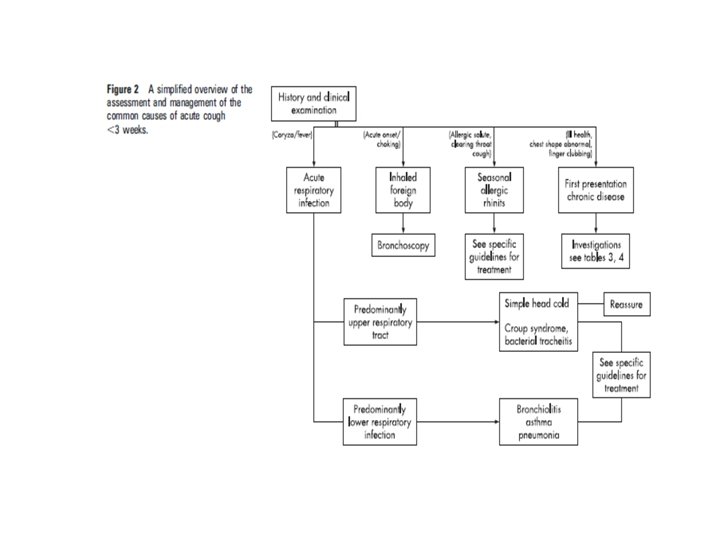
Acute cough (< 3 weeks) Feature Diagnosis • Snotty • Barking cough • Tachypnoea, resp distress, fever or focal signs • Paroxysmal/spasmodic • Sudden onset • Season • Other features (suggesting chronicity) • URTI • Croup/tracheitis • Pneumonia/Bronchiolitis/As thma • Pertussis • Foreign body • Allergic rhinitis • Underlying chest disease etc
URTI 7 -10 per year normal, often seasonal Resolve in between No abx, No linctus, ? salbutamol inhaler Education on cough durations 25% remain at 2 weeks, 10% at 4 weeks • The cough should be resolving!!! • • • If handing out salbutamol inhaler ensure max use 10 puffs 4 hourly (or less? )
Pertussis • Role for a macrolide abx early on • Whoop in older children only • Variable onset of cough, role of mobile video?
Allergic seasonal cough • Trial of nasal steroids or antihistamines reasonable
The Cx. R in acute cough • Fever/ Tachypnoea with nil else (esp toddler) or > 5 days • Unusual high fever with bronchiolitis • Relentless progressive • Foreign body (mention on the form!) • Suspect an acute on chronic presentation I do not perform a Cx. R to confirm diagnosis, but to make a diagnosis
Refer • • • Progressively worsening and serious cough Evolving sick child Foreign body Haemoptysis (rare) Instinct/other pathology concerns Review your decision/ arm parents with useful observations to make
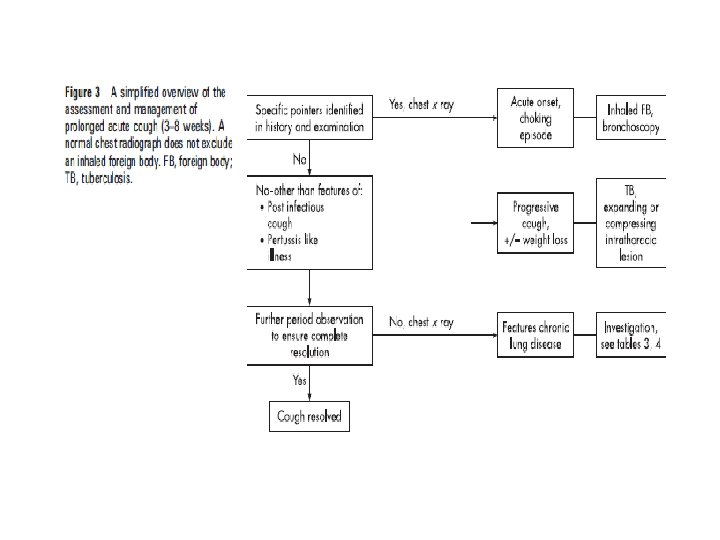
Prolonged acute/subacute cough (3 -8 weeks) • • • Grey area Still likely viral and pertussis aetiology Role for watchful waiting Actively follow up View as chronic cough if not abating Increasing role for Cx. R Consider measuring the child at this early stage to establish a baseline
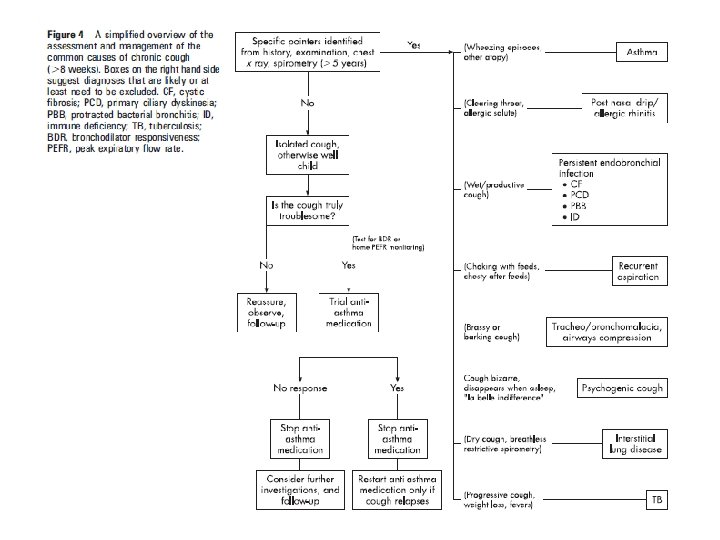
Chronic cough • Includes recurrent frequent cough (>2 URTI free episodes 7 -14 days apart in a year) • Stratify into normal child, specific cough and non specific isolated cough It would not have been unreasonable to have referred by this stage
Sadly it is not this simple
Detailed history Often easier stated than to do! Never unreasonable to re clarify!
How and when did the cough start? • Acute/sudden • Post URTI initially • Neonatal onset • FB? • Post infective (e. g. viral) • Congenital malformation (e. g. CCAM) • Primary Ciliary dysknesia • In utero lung infection • CF (rare nowadays)
What is the cough quality? • • Wet Paroxysmal Bizarre/dry/nil nocte Barking/dry • Haemoptysis (rare) Secretions Pertussis/parapertussis Habit/psychogenic Tracheal/Glottic ( e. g. malacia) • FB, CF, TB, Bronchiectasis, Tumour (all rare) • •
Is the cough an isolated symptom? • Associated ill health, recurrent pneumonia • Associated SOB • Wheeze present Immune deficiency, cilia disorders, bacterial bronchitis, FB Interstitial lung disease Asthma, FB, aspiration, malacia, interstitial lung disease, neonatal CLD
What triggers/exacerbates the cough? • Exercise, cold air • Asthma • Lying down • Postnasal drip, gastrooesophageal reflux, PBB • Feeding • Aspiration • ? Attention • ? Psychogenic
Other history of note Feature Consequence • FH atopy • Asthma more likely • DH • ACE inhibitor cough • Relentless and progressive • Lobar collapse, TB, tumour
Examination Clubbed Chest shape Asymmetric signs Ask child to cough Measure and plot height and weight • ENT • Skin • • •
Investigations • • • Cx. R useful to order at time of referral Consider spirometry Consider sputum sample (cough swab? ) Consider aeroallergen testing (RAST or SPT) Consider p. H probe/Barium swallow? ? ? I prefer the Cx. R only
Treatment options • Underlying diagnosis if specific cough otherwise…… • • Reduce/stop cigarette exposure Asthma therapy trial 8 weeks Watch and wait still Allergic rhinitis treatment? ? GORD? ? ? I am always interested in response to PO steroids (be generous)?
A recycled diagnosis – Protracted Bacterial Bronchitis (PBB) • Conducting airways disease – a biofilm disease • Role for temporary viral mediated cilia dysfunction? • Mainly children <6 years with persistent wet cough resolving briefly with antibiotics • Mimics asthma interval symptoms • “ 60 a day smoker cough”
Management dilemma • After referral please • Attempt an induced sputum sample • Unequivocal response to prolonged abx course • ? how long ( 2 weeks to resolution, then some more 6 -8 weeks) • Cross over with asthma? Concerns about abx over use.
A few sounds to finish off. • http: //children. webmd. com/pertussiswhooping-cough-10/coughing-sounds
Other resources/references • http: //www. britthoracic. org. uk/Portals/0/Guidelines/Cough/Guidelines/cough_in_children. pdf • http: //www. patient. co. uk/doctor/Chronic-Cough-in-Children. htm • http: //www. bmj. com/content/344/bmj. e 1177 • http: //n 3. learning. bmj. com/learning/module-intro/. html? module. Id=10032122 • http: //healthguides. mapofmedicine. com/choices/map/cough_in_children 1. html • http: //adc. bmj. com/content/98/1/72. abstract Protracted bacterial bronchitis
Questions