Autoimmune Hepatitis Amany Saleh ELYAMANY Assistant Professor of

 is a generally unresolving inflammation of the liver of unknown cause.")

, and an acute severe presentation, characterized")


 – Alcoholic")

 have been recognized")
; these include autoimmune thyroid disease, synovitis,")




.")










- Slides: 29
Autoimmune Hepatitis Amany Saleh ELYAMANY Assistant Professor of Hepatology Internal Medicine Department Alexandria University
Autoimmune hepatitis (AIH) is a generally unresolving inflammation of the liver of unknown cause. its pathogenesis postulates: Environmental triggers Failure of immune tolerance mechanisms Genetic predisposition …… T cell–mediated immune attack upon liver antigens, leading to a progressive necroinflammatory and fibrotic process in the liver.
Onset is frequently insidious with nonspecific symptoms such as: fatigue, jaundice, nausea, abdominal pain, and arthralgias at presentation. The clinical spectrum is wide, ranging from an asymptomatic presentation to an acute severe disease.
An acute onset of illness is common (40%), and an acute severe presentation, characterized by hepatic encephalopathy within 8 weeks of clinical symptoms, is sometimes seen
The diagnosis is based on histologic abnormalities, characteristic clinical and laboratory findings, abnormal levels of serum globulins, and the presence of one or more characteristic autoantibodies. Women are affected more frequently than men (sex ratio, 3. 6: 1). the disease is seen in all ethnic groups and at all ages
§ Autoantibodies – ANA, ASMA, LKM-1, SLA § Ig. G – Typically elevated in autoimmune hepatitis § Histology – Interface hepatitis, lymphocytic or lymphoplasmacytic infiltrate, rosettes § Exclusion of viral hepatitis – Hepatotropic viruses and others Hennes et al. Hepatology 2008; 48: 169
§ Exclusion of other chronic diseases – Viral hepatitis (HBV and HCV) – Alcoholic liver disease and NAFLD – Drug-induced hepatotoxicity – Wilson disease – Hereditary hemochromatosis – Alpha-1 -antitrypsin deficiency – Primary biliary cirrhosis – Primary sclerosing cholangitis
Liver biopsy examination at presentation can establish the diagnosis and guide the treatment decision. In acute presentation unavailability of liver biopsy should not prevent from start of therapy. Interface hepatitis is the histological hallmark , and plasma cell infiltration is typical. Neither histological finding is specific for AIH, and the absence of plasma cells in the infiltrate does not preclude the diagnosis. Eosinophils, lobular inflammation, bridging necrosis, and multiacinar necrosis may be present
Autoantibody Classification Two types of AIH (type 1 and type 2) have been recognized based on serological markers but have not been established as valid clinical or pathological entities. A proposed third type (type 3) has been abandoned, as its serologic marker (anti-SLA) is also found in type 1 AIH and in type 2 AIH. Type 1 AIH is characterized by the presence of ANA, SMA or both, and constitutes 80% of AIH cases. Seventy percent of patients are female, with a peak incidence between ages 16 and 30 years.
Associations with other autoimmune diseases are common (15%-34%); these include autoimmune thyroid disease, synovitis, celiac disease, and ulcerative colitis. At the time of diagnosis, cirrhosis is present in 25% of patients. Antibodies to SLA have emerged as possible prognostic markers that may identify patients with severe AIH who are prone to relapse after corticosteroid withdrawal.
Type 2 AIH is characterized by the presence of anti. LKM 1. Most patients with type 2 AIH are children, and serum immunoglobulin levels are usually elevated Concurrent immune diseases are common, progression to cirrhosis occurs, and an acute severe presentation is possible.
Other acute and chronic liver diseases of diverse etiologies that can have serological features of AIH include alcoholic and nonalcoholic fatty liver disease, acute and chronic viral hepatitis, and drug induced hepatitis. Drugs such as diclofenac, infliximab, propylthiouracil, atorvastatin, nitrofurantoin, methyl dopa, and isoniazid can cause a syndrome that resembles AIH replete with autoantibodies that generally disappear after discontinuation of the drug. Similarly, an AIH-like clinical syndrome has been associated with various herbal medications and with vaccination
Extrahepatic Autoimmune Diseases • Autoimmune thyroiditis • Grave’s disease • Connective tissue diseases • Inflammatory bowel disease • Celiac disease • Adrenal insufficiency • Autoimmune hematologic disorders • Type 1 DM • Sjogren’s syndrome • Fibrosing alveolitis • Vitiligo • Vasculitis • Nephritis
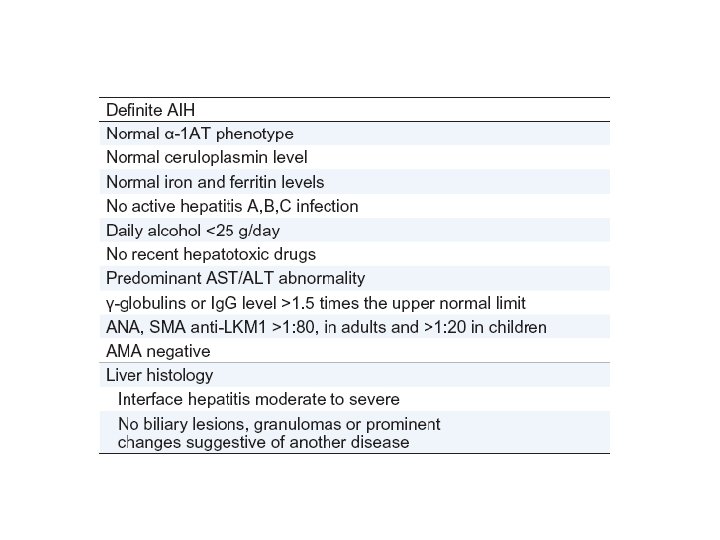
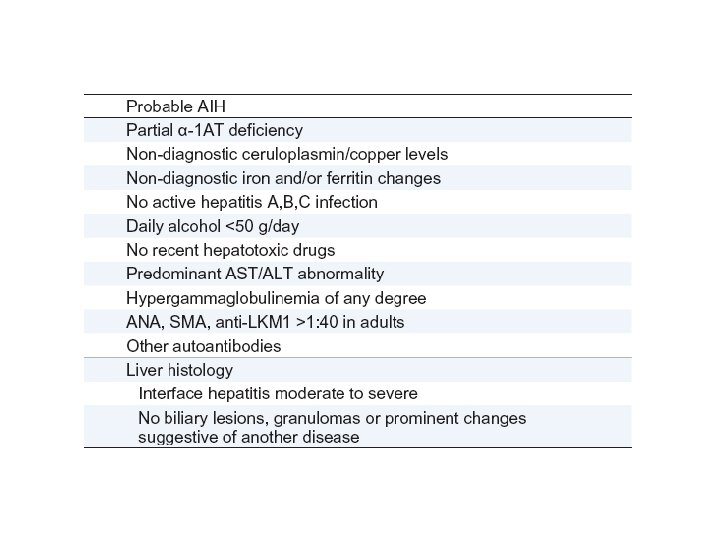
Simplified diagnostic criteria of the International Autoimmune Hepatitis Group Definite AIH: ≥ 7, Probable AIH: ≥ 6
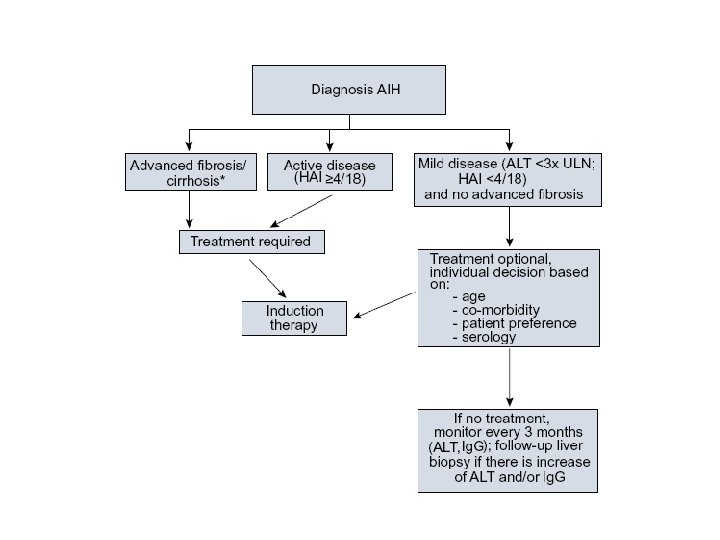
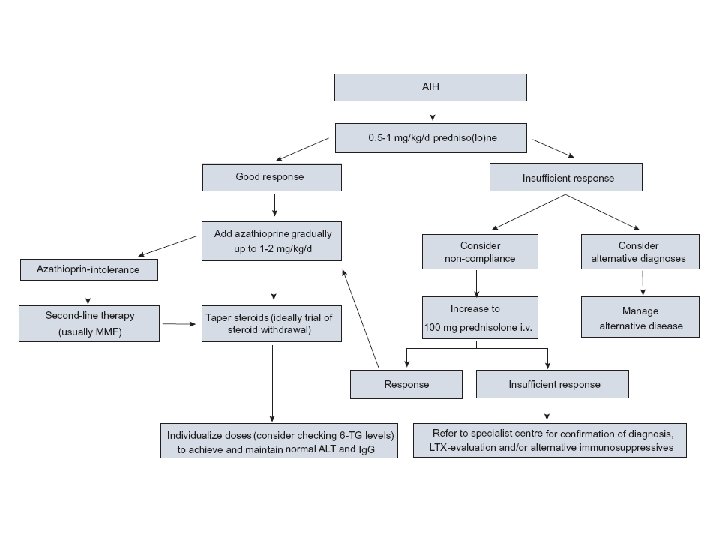
Treatment proposal for adult patients with AIH (e. g. 60 kg).
Follow-up of autoimmune hepatitis patients who have achieved remission.
Treatment should be continued for at least three years and for at least 24 months after complete normalisation of serum transaminases and Ig. G levels (biochemical remission). Performance of a liver biopsy prior to treatment withdrawal is advisable as histological findings are predictive of fibrosis progression and relapse
Immunosuppressive treatment should be instituted in patients with serum AST or ALT levels greater than 10 -fold ULN, at least five-fold ULN in conjunction with a serum c -globulin level at least 2 - fold ULN, and/or histological features of bridging necrosis or multilobular necrosis
Immunosuppressive treatment may be considered in adult patients without symptoms and mild laboratory and histological changes, but the decision must be individualized and balanced against the possible risks of therapy
Immunosuppressive treatment should not be instituted in patients with minimal or no disease activity or inactive cirrhosis, but these patients must continue to be followed closely, i. e. , 3 -6 months
Immunosuppressive treatment should not be instituted in patients with serious pre-existent comorbid conditions (vertebral compression, psychosis, brittle diabetes, uncontrolled hypertension), or previous known intolerances to prednisone unless the disease is severe and progressive and adequate control measures for the comorbid conditions can be instituted
Azathioprine treatment should not be started in patients with a severe pretreatment cytopenia (white blood cell counts below 2. 5 or platelet counts below 50 )
Immunosuppressive Therapy § Prednisone – 30 mg/d x 1 week – 20 mg/d x 1 week – 15 mg/d x 2 weeks – 10 mg/d until endpoint § Azathioprine – 50 mg/d until endpoint § Prednisone alone – 60 mg/d x 1 week – 40 mg/d x 1 week – 30 mg/d x 2 weeks – 20 mg/d until endpoint
Alternative Medications § § § Mycophenolate Cyclosporine Tacrolimus Budesonide Methotrexate Cyclophosphamide
• Chronic hepatocellular disease of unknown etiology • Clinical presentation is variable • Diagnosis based upon LFTs, serology, gamma globulins, and histology • Immunosuppressive therapy is the mainstay of treatment • Tailor therapy based upon treatment endpoints