Anatomical aspect of pericarditis cardiac tamponade and paracentesis














 Vasodilation: transudation of fluid 2) Increased vascular permeability leakage of protein 3)")





- Slides: 22
Anatomical aspect of pericarditis, cardiac tamponade and paracentesis
Heart enclosed within the pericardial sac is located in the middle mediastinum
Mediastinum: Divisions Divided, by an imaginary plane passing from the sternal angle anteriorly to the lower border of the body of the 4 th thoracic vertebra posteriorly, into: • Superior mediastinum • Inferior mediastinum The inferior mediastinum is further divided into: • Anterior • Middle • Posterior
Pericardium
Pericardium Double layered fibroserous sac that encloses the heart & the roots of the great vessels Located in the middle mediastinum § Posterior to the body of sternum and 2 nd-6 th costal cartilages § Anterior to T 5 -T 8 vertebrae § 1 -1. 5 cm to the right of the sternum § 5 -7. 5 cm to the left of median plane at the level of 5 th intercostal space
Pericardium cont’d The strong outer layer, the fibrous pericardium is composed of tough fibrous tissue The inner transparent membrane, the serous pericardium, has two layers: • Parietal • Visceral
Fibrous Pericardium Tough conical outer fibrous sac, protects heart against sudden overfilling Superiorly: § Pierced by aorta, pulmonary trunk, and superior vena cava § Becomes fused with the tunica adventitia of these vessels Below: rests on and is fused with the central tendon of the diaphragm
Fibrous Pericardium cont’d Anteriorly attached to the posterior surface of sternum by condensations of connective tissue called the sternopericardial ligaments Posteriorly: § Pierced by pulmonary veins and inferior vena cava § Becomes fused with the tunica adventitia of these vessels
Serous Pericardium Parietal layer lines the fibrous pericardium and becomes continuous with the visceral layer around the roots of great vessels Visceral layer reflected onto the heart, forms the external layer of the heart wall (epicardium) The two layers are continuous with each other at the base of the large vessels Pericardial cavity lies between the two layers, that contains a thin film of serous fluid which helps in frictionless movement of the heart
Pericardial Sinuses Develop during folding of embryonic heart Transverse sinus: § Lies posterior to ascending aorta and pulmonary trunk, anterior to superior vena cava § Communicates with the main part of pericardial cavity at its right and left ends Oblique sinus: § An inverted U-shaped blind recess lies posterior to the heart extending posterior to the left atrium, can be entered inferiorly § Produced by the reflection of pericardium onto the pulmonary veins and inferior vena cava
Blood Supply Arterial Supply: • Fibrous pericardium & the parietal layer of the serous pericardium : Mainly supplied by pericardiophrenic and musculophrenic arteries, branches of internal thoracic. Also supplied by pericardial branches of bronchial, esophageal and superior phrenic arteries • Visceral layer of the serous pericardium (epicardium) supplied by the branches of the coronary arteries Venous drainage: Veins are tributaries of azygos system. Pericardiophrenic veins also drain into the internal thoracic vein
Nerve Supply The fibrous pericardium and the parietal layer of the serous pericardium are supplied by the phrenic nerves. The visceral layer of the serous pericardium is innervated by sympathetic & parasympathetic fibers through the sympathetic trunks and the vagus nerves respectively
Clinical Notes Pericarditis & pericardial effusion Cardiac temponade Pericardiocentesis:
Pericarditis Inflammation of pericardium I. INFECTIVE II. AUTOIMMUNE DISORDERS III. NEOPLASM IV. RADIATION PERICARDITIS V. RENAL FAILURE (uremia) VI. TRAUMATIC CARDIAC INJURY VII. IDIOPATHIC
Pathogenesis 1) Vasodilation: transudation of fluid 2) Increased vascular permeability leakage of protein 3) Leukocyte exudation neutrophils and mononuclear cells Pathology depends on underlying cause and severity of inflammation serous pericarditis serofibrinous pericarditis suppurative (purulent) pericarditis hemorrhagic pericarditis
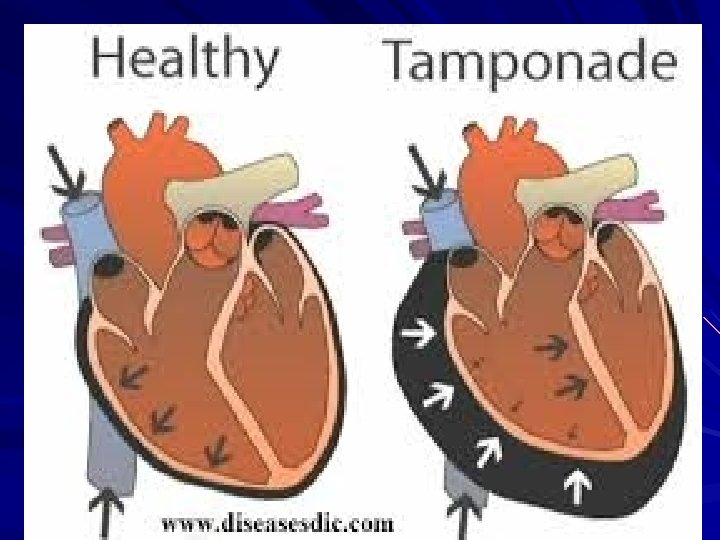
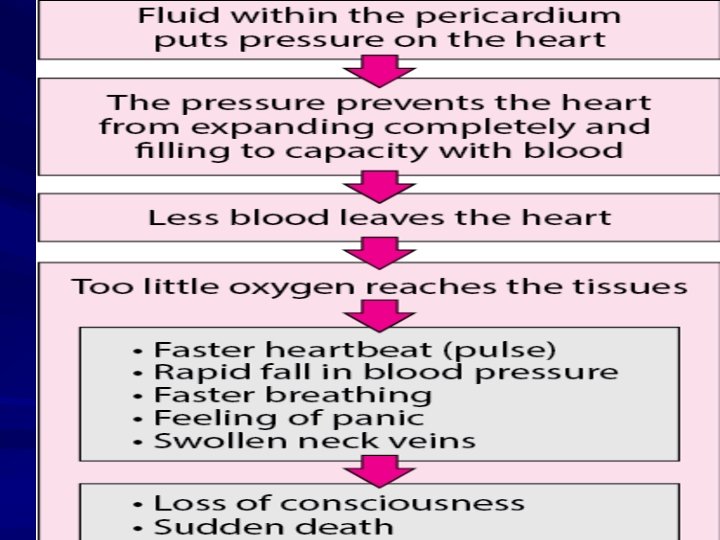
Cardiac Tamponade Fluid under high pressure compresses the cardiac chambers: acute: trauma, LV rupture – may not be very large gradual: large effusion, due to any etiology of acute pericarditis
Pericardiocentesis
Approaches 1 -Apical 2 -Subxhiphoid 3 -Parasternal approach Indications 1 -cardiac tamponade 2 -Pericarditis with pericardial preasure >20 mmhg on echocardiography
Different approaches
Thank U & Good Luck