3 studies noncardiac surgery in patients with IHD


 – Simple – widely used")







")













- Slides: 32
3 studies noncardiac surgery in patients with IHD • In surgical patients > age 40 : • Perioperative MI : 1. 4 % • Cardiac death : 1. 0 %. • With some selection criteria : • Perioperative MI : 3. 2 % • cardiac death : 1. 7 %. • MACE in large administrative database : • death, acute MI, or acute ischemic stroke : 3%
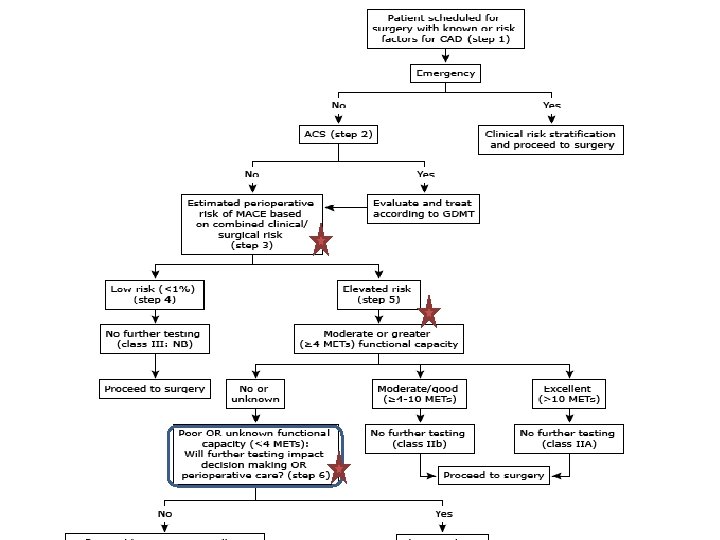
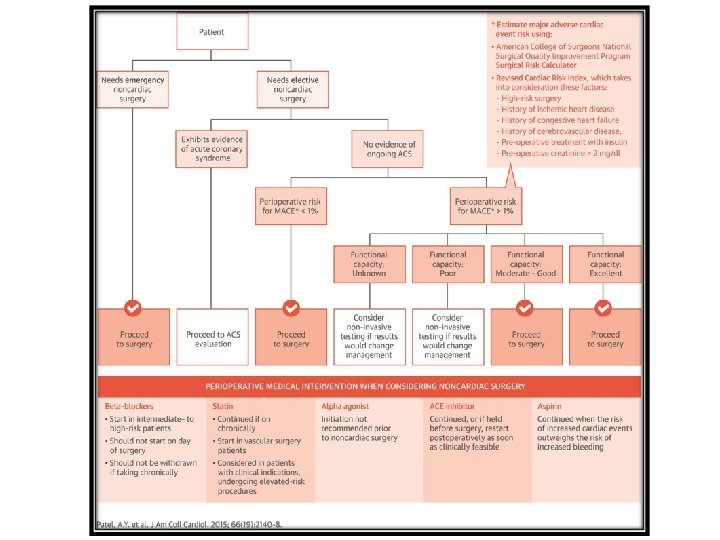
Risk prediction of perioperative cardiac event Ø an initial estimate of perioperative cardiac risk with : • History & physical examination, • Type of surgery Ø Weigh the benefits and risks of the surgery. Ø optimize the timing of the surgery. Ø uncover undiagnosed or suboptimally treated conditions.
Risk stratication models • revised cardiac risk index (RCRI) – Simple – widely used – Validated (over the past 15 years). • Lee index • American College of Surgeons National Surgical Quality Improvement Program (NSQIP) – more complex – requiring calculator (online tool). – A simpler tool also derived from the NSQIP : Gupta myocardial infarction or cardiac arrest (MICA)
RISK factors in RISK prediction MODELS ü ü ü ü ü Surgery-specific risk (RCRI and NSQIP) History of ischemic heart disease (RCRI). History of heart failure (RCRI). History of cerebrovascular disease (RCRI). Insulin dependent diabetes mellitus (RCRI). Serum creatinine ≥ 2. 0 mg/d. L (RCRI) or >1. 5 mg/d. L (NSQIP). Increasing age (NQSIP). American Society of Anesthesiologist class (NSQIP). Preoperative functional status (NSQIP). ü Atrial fibrillation & Obesity
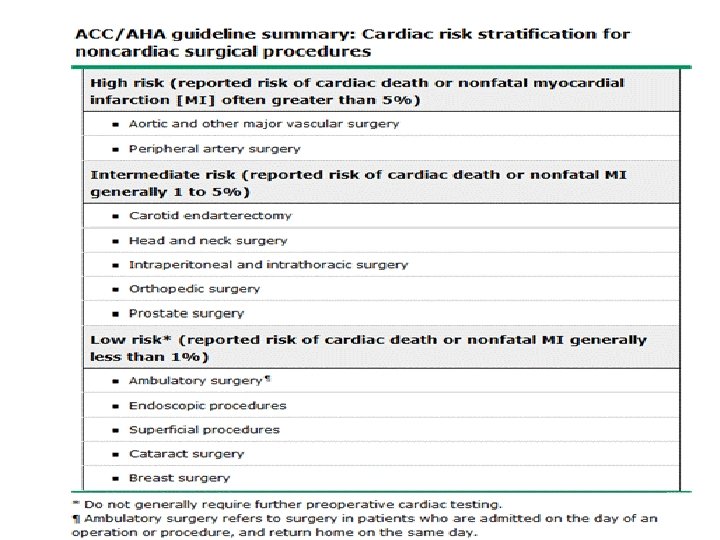
Surgery-specific risk • Institutional and/or individual surgeon experience • Emergency surgery : cardiac complications are 2 -5 times more likely than elective procedures. • Type of surgey
Copyrights apply
Copyrights apply
Gupta MICA NSQIP database risk model Five factors were identified as predictors of MI or cardiac arrest : ●Type of surgery. ●Dependent functional status. ●Abnormal creatinine. ●American Society of Anesthesiologists class. ●Increased age. An easy-to-use calculator was developed from this model.
Copyrights apply
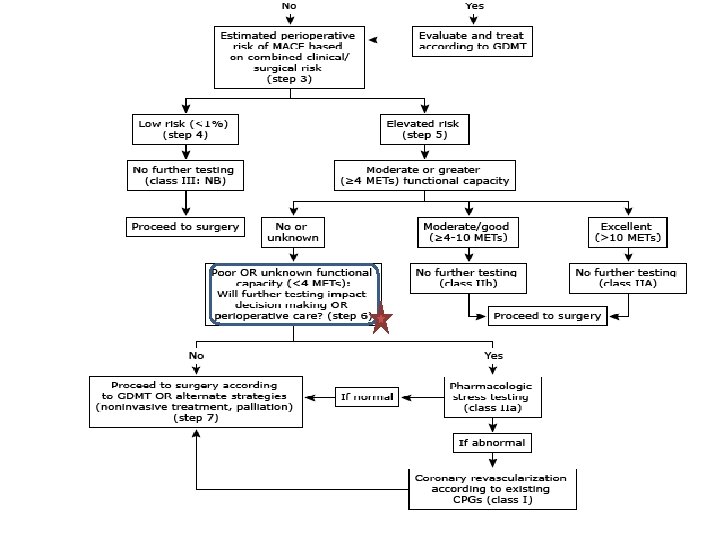
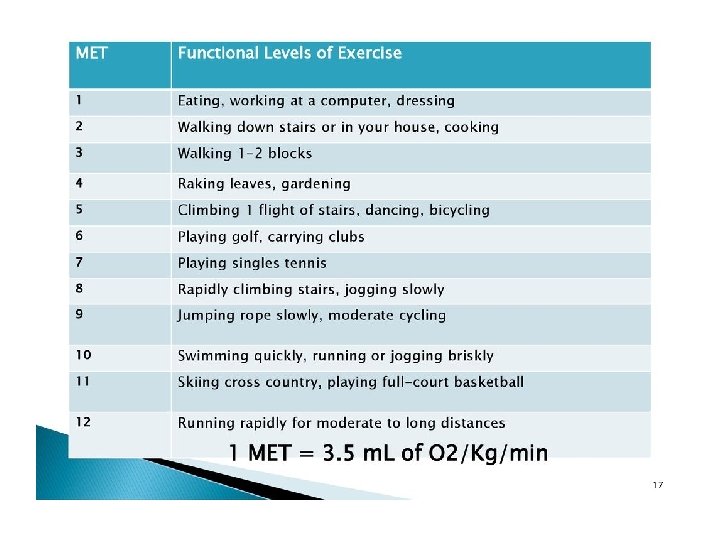
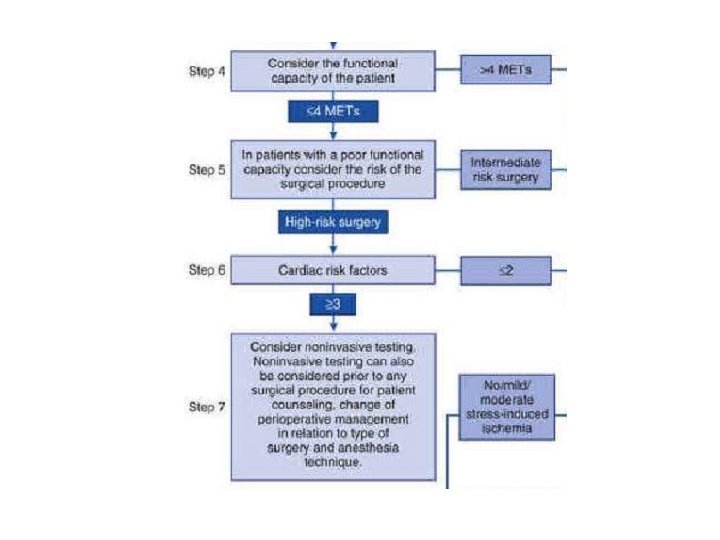
1 MET : 3. 5 cc O 2 uptake/kg /min oxygen uptake in a sitting position ü Can take care of self, such as eat, dress, or use the toilet (1 MET) ü Can walk up a flight of steps (a flight of stairs has 12 or 13 steps. )or a hill or walk on level ground at 6 Km/h (4 METs) ü Can do heavy work around the house, such as scrubbing floors or lifting or moving heavy furniture, or climb two flights of stairs (between 4 and 10 METs) ü Can participate in strenuous sports such as swimming, singles tennis, football, basketball, and skiing (>10 METs).
Refer to cardiologist : if patients assessed to be at elevated (intermediate or high) cardiovascular risk. PATIENTS WHO NEED URGENT OR EMERGENT SURGERY & known or suspected CAD , HF or VHD urgent consultation with a cardiologist. Additional testing will not be performed But suggestions about : monitoring and medication management during & after the procedure.
preoperative ECG • Asymptomatic patients without known CVD: rarely helpful. • ECG abnormalities are not part of (RCRI) or (NSQIP) The rationale for a preoperative baseline ECG : comparative postoperative ECG abnormalitis.
FURTHER CARDIAC TESTING • Only if it is indicated in the absence of proposed surgery. • There is no evidence that further diagnostic or prognostic evaluation improves surgical outcomes. • Preoperative cardiac evaluation and testing may differ for patients being evaluated for liver or kidney transplant.
Resting echocardiography • Is not indicated : unless there is another indication, such as : – Murmur – Dyspnea of unknown cause – Edema.
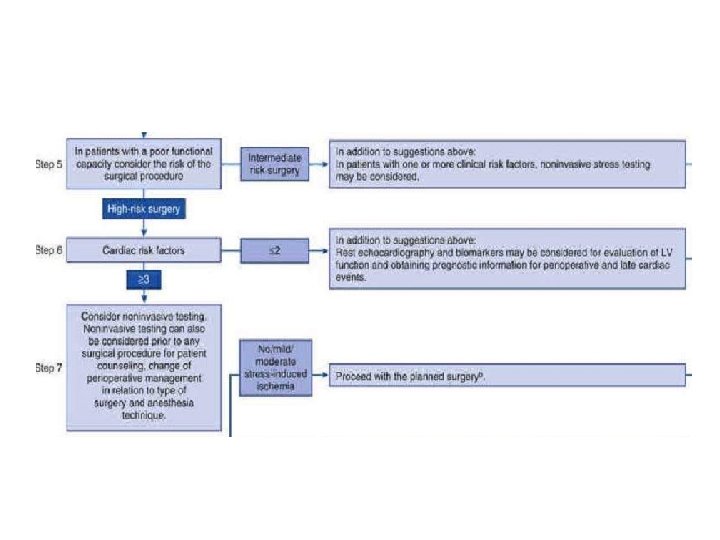
Stress testing • Is not indicated : solely because of the surgery if there is no other indication. • Some experts : routine preoperative stress imaging in major vascular surgery • No evidence for: prophylactic revascularization to prevent ischemia & improves outcomes.
Revascularization before surgery • Except in ACS : myocardial revascularization prior to noncardiac surgery is not recommended. • Patients with stable CAD do not benefit from prophylactic revascularization prior to noncardiac surgery. • only patients with unprotected left main benefited from preoperative revascularization (high risk non-invasive tests).
“ Stents “ Perioperative DAPT & Bleeding • The proinflammatory and prothrombotic condition up to 1 M. after surgery (regardless of stent type)may increase the baseline risk of stent thrombosis. • aspirin alone (20%) & with P 2 Y 12 blocker (50%) increases the risk of bleeding. • increase in PC transfusion, but not in surgical mortality or morbidity.
premature cessation of DAPT • The major predictor of stent thrombosis, irrespective of stent type. • The risk has been estimated to be 30 - to 50 -fold or greater. • In patients who stop both agents, stent thrombosis generally occurs within 10 days in the majority of patients.
2016 ACC guideline
Non-emergent noncardiac surgery • Defer surgery until six months for BMS and DES. • patients whose essential surgery cannot wait : minimal duration of DAPT is three months for both BMS and DES. • Before 3 M. : – In many cases : DAPT can be continued in the perioperative period. – In some such as neurosurgery, posterior eye or prostatic surgery , the risk of major bleeding may be greater than the risk of stent thrombosis. – P 2 Y 12 receptor blocker should be discontinued for as brief a period as possible. – Aspirin should be continued & surgery can generally usually be safely performed on aspirin(POISE-2) (neurosurgery? !).
Non-emergent noncardiac surgery • Minor surgical and dental procedures usually do not require DAPT cessation • Clopidogrel 5 , prasugrel 7 and ticagrelor 3 -5 days should be stopped, before surgery. • shorter discontinuation periods : for procedures less likely to be associated with bleeding. • Clopidogrel, if stopped, should be restarted with a loading dose of 300 even 600 mg. • Surgery should be performed in centers with 247 centers.
Urgent or emergent noncardiac surgery • The relative risks and benefits of continuing DAPT (!!) • Role of platelet transfusion (? ? ). • when antiplatelet therapy must be stopped (neurosurgery ), defer surgery for at least 48 hours after angioplasty.
Potential ALTERNATIVES to DAPT • tirofiban or eptifibatide are under investigation. • Ticagrelor (a reversible platelet inhibitor with a shorter half-life) can be stopped as late as 48 hours before surgery.