24 may 2006 King Faisal University College of









 It is")










 2 -")


















 : Leukocytes Count especially neutrophiles ü Urine")







- Slides: 49
24. may. 2006 King Faisal University College of Medicine Surgery I 4 th year Done by: Fatima A. Al-Hashim Iman Al-Mukhtar Supervised by: Dr. A. Al-Mulhim Dr. H. Wadani
Introduction History taking Anatomy Physical examination Etiology Preoperative complication pathogenesis Investigation Signs & Symptoms Differential Diagnosis Appendectomy Postoperative complication
Introduction
What is appendicitis? ? Appendicitis is the inflammation of appendix. Øappendicitis is the most common cause of the intra -abdominal infection in developed countries. Ø &it is the most common emergency surgical operation Øappendicitis can occur at any age but is most common below 40 yrs , especially between the ages of 8 & 14 yr &it is very rare below the age of 2.
Anatomy
Site Rt iliac fossa , attached to the posteromedial aspect of caecum 2 cm below the iliocaecal valve. Size 2 -20 cm long (average 10 cm) & about 12 cm wide Peritoneal covering of the appendix It is completely covered with peritoneum & is suspended to the back of the mesentery of terminal ileum by a triangular fold of peritoneum called mesoappendix
Nerve supply T 10 supplies the peritoneal covering of the appendix referred pain of the appendix is felt at the umbilicus which has the same nerve supply. Venous drainage appendicular vein ileocolic vein superior mesenteric vein portal vein Arterial supply: Appendicular artery Branch of ilio-colic artery It runs in the free border of the mesoappendix towards the tips.
Position The base of the appendix is fixed , its tip points to one of the following positions 1 - Retrocecal ( 74% ): behined the caecum ( in the retrocaecal recess) 3 -subcaecal (3. 5%): the appendix lies below the caecum. 5 -post-ileal (12 %): the appendix lies behined the terminal part of ileum, in contact with the ileocolic V. it is the most dangerous position because spread of the infection to the vien may lead to portal pyaemia. 2 -pelvic (21%): the appendix hangs over the pelvic brim where it is related to external iliac vessels , ovary & uterine tube. 4 -pre-ilial (1%): infront of the terminal part of the ileum
ØMicroscopically the submucosa of the appendix is rich in lymphoid tissue ØIdintification of appendix at operation inside the abdomen the base of the appendix is easly found by identifying the tenia coli of the cecum & following them to the base of the appendix where they coverage to form complete longitudinal muscular coat Øconginital abnormalities 1 -absence of appendix (agenesis-) 2 -double appendix 3 -appendix lying in the Lt iliac fossa-
Surface anatomy of the base of appendix ( Mc. Burney's point ) It is a point at the junction of the lateral 13 & medial 23 of a line extending from the anterior superior iliac spine to the umbilicus (spinoumbilical line)
Etiology
Infection of appendix by 2 routs hematogenous endogenous common rare obstructed By: 1 -faecolith commonest 2 -foreign body 3 -lymphoid hyperplasia due to viral infection 4 -stricture 5 -carcinoid tumor 6 -chron's disease 7 -parasetic infection particularly by oxyuris vermicularis (pin warm) non-obstructed appendix due to direct infection of lymphoid follicle from appendicular lumen
pathogenesis
bacterial flora located within the lumen of appendix include both obstructed appendix aerobic & anaerobic organism typical of those found in the large intestine stasis prolofiration of the gas forming bacteria increase intralumenal pressure acute inflamation of mucosa acute appendicitis with edema , lymphoid obstruction, & necrotizing ulceration of the mucosa
If the diagnosis of appendicitis is not made early the process will continue
extension of inflammation across appendicael wall involvment of serosa by inflammation visceral peritonitis obstruction of venous & lymphatic drainage & arterial thrombosis Gangrene of appendix wall perforation
the outcome of perforation depend on the ability of the omentum to contain the infection Inadequate omemtum generalized peritonitis apendicular mass or abcess will result
Symptoms
Common symptoms: 1 -Abdominal pain Periumblical pain migrate to Rt lower quadrent 2 -Anorexia 3 -Nausea 4 -Vomiting 5 -low-grade fever
Signs
1 -Right lower quadrant pain on palpation (the single most important sign) 2 - Low-grade fever (38°C [or 100. 4°F]) absence of fever or high fever can occur -3 -Localized tenderness to percussion 4 -Guarding 5 -Other confirmatory peritoneal signs (absence of these signs does not exclude appendicitis) • Psoas sign • Obturator sign • Rovsing's sign • Dunphy's sign--increased pain with coughing • Flank tenderness in right lower quadrant
Differential Diagnosis
Children -Gastroenterits -Mesenteric adenitis -Meckel`s diverticulitis -Intussusception -Lobar pneumonia Elderly -Sigmoid diverticulitis -Intestinal obstruction -Colonic carcinoma -Mesenteric infarction -Aortic aneurysm
Adult male -Regional enteritis -Ureteric colic -Perforated ulcer -Torsion testis -Pancreatitis -Rectus sheath hematmoa Adult female -Salpingitis -Pyelonephritis -Ectopic pregnancy -Torsion/rupture of ovarian cyste -Endometriosis
History Taking
The components of the surgical history are that of any other history, including; üAn introduction üPresenting complaint üHistory of presenting complaint üPast history ( medical & surgical ) üDrugs/allergies üFamily history üSocial history üOccupational history üSystems enquiry
Age & Sex : Appendicitis does occur at any age but most often affects young adults or teenagers of either sex. Ask about üThe site of the pain üOnset üSeverity üPattern üIs it localized in a particular area or not üRadiation üDuration üProgression üAggregating Factors ü Relieving Factors üAssociated Symptoms
Physical examination
üGeneral Appearance : Patient looks unwell with flushed cheeks Tongue “ white & furred with foetor oris “ Pale ( especially in children ) Tachycardia Low grade fever ü Head & Neck : Observe the tonsils & Palpate the lymph nodes
üChest : Examine the Lungs ü Abdomen : • Inspection Usually normal shape , the abdomen is slowly moves with respiration due to pain • Palpation The Rt iliac fossa is tender with or without guarding Rebound Tenderness: +ve in Mcburneys point
ü Signs : I- Rovsing`s sign : Pain in the Rt iliac fossa on palpation or percussion on Lt iliac fossa. II- Psoa`s sign : Pain when extending the Rt hip joint due to spasm of the psoa`a muscle.
The psoas sign. Pain on passive extension of the right thigh. Patient lies on left side. Examiner extends patient's right thigh while applying counter resistance to the right hip asterisk Anatomic basis for the psoas inflamed appendix is in a sign: retroperitoneal location in contact with the psoas muscle, which is stretched by this maneuver
III-Obturator`s sign : Pain with passive internal rotation of the flexed Rt thigh it indicated inflammation overlying that muscle.
IV-Blumberg`s sign : Crossed Rebound tenderness in the Rt iliac fossa after pressing and sudden release on Lt iliac fossa. V-Straight leg arising sign : +ve in retrocecal appendix
üRectal Examination : Tenderness in pelvic appendix or if there is inflammation or pus in Douglas pouch
Preoperative complication
Systemic Complications : ü Acute toxemia ü Septicemia ü Portal pyemia
Local Complications : ü Appeddicular Abscess ü Appedidicular fistula ü Rupture supportive peritonitis ü Turns to chronic appendicitis
Investigation
ü Complete Blood Count ( CBC ) : Leukocytes Count especially neutrophiles ü Urine Analysis Albuminuria , Hematuria (25 -40% of patient). üPlain X-ray ü Ultra Sound ü CT scan
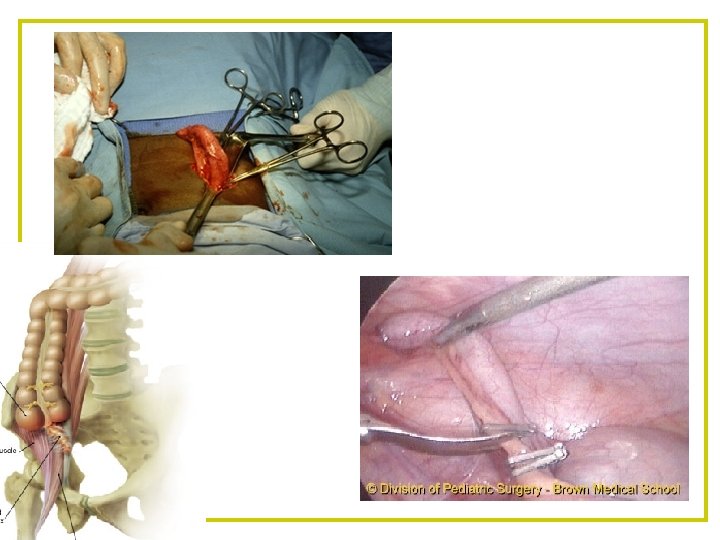
Appendectomy
üConventional Open Operation §Grid-iron incision §Lower midline abdominal incision ü Laparoscopic Technique
ü A normal appendix is found ü The Appendix can not be found ü An Appendicular Tumor is found ü An Appendix Abscess is found
Postoperative complication
Postoperative complication ü Wound Infections ü Intra-abdominal Abscesses ü Venous Thrombus & Embolism ü Portal Pyemia ( Pylephlebitis ) ü Faceal Fistula ü Adhesive intestinal obstruction ü Right inguinal hernia
üAntibiotic prophylaxis ü If perforation has occurred, IV antibiotics should be continued for 5 -10 days.