Anticoagulation in HD Faisal Zidan Consultant nephrologist Shirbin

Anticoagulation in HD Faisal Zidan Consultant nephrologist Shirbin General Hospital

History of Anticoagulation • Abel 1914 : First efficient dialysis system in animal consist of collodion tubes and hirudin solution used as anticoagulant. • Hess and Mc. Guigan 1914 : clotting is avoided by high blood flows or anticoagulation. • Haas 1924 : first human hemodialysis in Germany using a tubular device made of collodion and hirudin for anticoagulation. • 1930 s : Unfractionated heparins. • 1940 s : Vitamin K antagonists.

History of Anticoagulation • 1980 s : LMWH. • 1990 s : Direct factor IIa inhibitors (Parentral). • 2000 s : Indirect factor Xa inhibitors (Parentral). Direct factor IIa inhibitors (Oral). • 2008 : Direct factor Xa inhibitors (Oral).

Coagulation factors

Pumb UF

Types of anticoagulants • • • UFH LMWH Regional citrate Heparinoids Direct thrombin inhibitors Platelet inhibiting agents

UFH § Glycosaminoglycan extracted from bovine or porcine tissues § Half-life 30– 120 min. § Monitoring : ü ACT : (200– 250 s) during dialysis (150– 200 s) during last 60 min. of dialysis ü APTT : (target 120– 160 s). § Binds antithrombin III to inactivate factors II, IX, X, XI, and XII.

Mechanism of action of UFH

UFH
 q Infusion method")
Heparin administration (There are no good evidence demonstrating the best method) q Infusion method : Initial bolus usually 2000 U. Continuous infusion 500– 2000 U/h. Adjust infusion rate to clotting time. Stop heparin 1 h. before end of dialysis. q Bolus method: Initial bolus 1000– 4000 U. Repeat ACT in 30 min & give other bolus accordingly. Stop heparin 1 h. before the end of dialysis. q Tight (or minimal) heparin : Initial bolus (750 U) followed by 500 U bolus every 30 min. or 250 : 500 U/h. by infusion & continue till the end of HD.

§ Side efects include: ü Major complication is bleeding (in up to 50% of high risk patients). ü Heparin-induced thrombocytopenia (HIT) ü Pruritus ü Thrombocytopenia (rare in HD) ü Hyperlipidaemia (mainly hypertriglyceridaemia) ü Osteoporosis ü Hair loss ü Allergy (rare).

LMWH Enoxaparin, Nadroparin, Tinzaparin, Deltaparin & Reviparin Obtained by fractionation of heparin. Binds anti-thrombin III and inhibits factor Xa. Monitored by the anti-factor Xa activity in plasma. Cleared by renal/dialysis mechanisms, so dosage must be adjusted. • Given as single dose ( may be repeated). • •
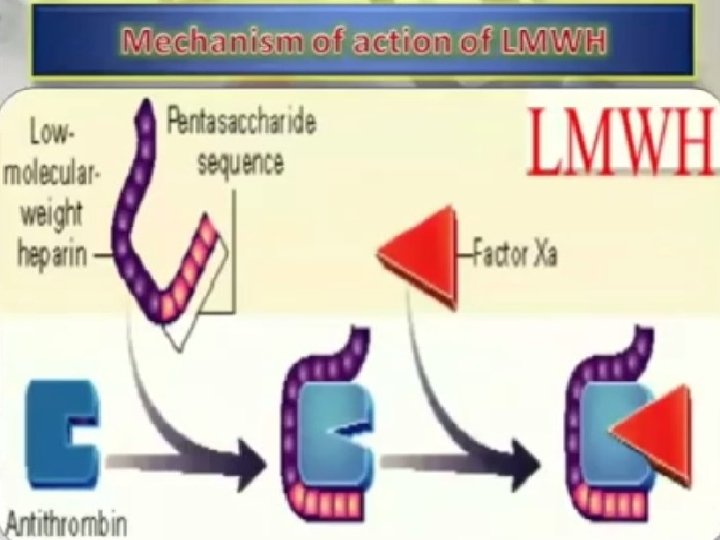

LMWH

Doses of LMWH in IHD

UFH vs LMWH UFH LMWH MW 5000 : 40000 Da. 2000 : 9000 Da. Onset of action Slower More rapid Duration of action Short Long Bioavailability Less More Monitoring ACT & APTT Anti- Xa level Frequent monitoring Needed Not needed Antidot Protamine No Convenience Less More Nursing demand More Less HIT More Less Plt. & Leucocytes activation More Less Osteoporosis More Less Alopecia More Less Dyslipidemia More Less K & Aldosterone More Less Cost Cheep Expensive

UFH vs LMWH

No significant differance

No significant differance

Heparin-coated dialyzer

Heparin-free dialysis Indications: • Actively bleeding patients. • Pericarditis. • Coagulopathy. • Thrombocytopenia. • Intracerebral haemorrhage. • Recent surgery. • Recent renal transplant.

Heparin-free dialysis Common protocol § § § § Rinse circuit with heparinized saline (2000– 5000 U/L saline). Use high blood flows (>400 m. L/min). Rinse circuit every 15– 30 min with 25– 200 m. L saline. Only 5% risk of complete circuit Increase UF rate to remove extra saline. Careful inspection of dialyser. clotting. Monitoring of venous pressure for early signs of clotting. Avoid blood transfusion. Use predilution CRRT. Requires more intensive nursing.

Regional anticoagulation • Regional heparin with protamine reversal • Heparin is infused constantly into the dialyzer inlet & protamine is infused into the venous line. • Protamine binds heparin and prevents its anticoagulant activity. • ACT is maintained in the circuit at 200– 250 s, and also monitored in the blood returning to the patient (should be back to baseline). • 1 mg protamine reverses 100 U of heparin. • This is difficult to monitor. • Rebound bleeding can occur after 2– 4 h (Can be severe). • Protamine can cause flushing, hypotension and bradycardia. Rarely used now

Heparin regional anticoagulation

Regional anticoagulation • Regional citrate anticoagulation • Baseline ACT is measured and then every 30 min. (100% above baseline or 200 s) • Trisodium citrate solution (132 mmol/L) is infused into the Where routinely used it is a reliable and arterial line at 270 m. L/h effective means of anticoagulation • Start blood flow • Start calcium chloride infusion into venous line at 30 m. L/h • Titrate calcium infusion to plasma calcium level • Ensure neither citrate nor calcium pumps stop working during the procedure • Stop both calcium and citrate infusions at the end of dialysis. • Hypocalcaemia, hypernatraemia and metabolic alkalosis are possible complication.

Regional citrate anticoagulation

Citrat

1051 session : 3 clottings

Decreased KT/V Hypocalcaemia

Heparinoids Danaparoid & Fondaparinux • Mixture of heparin, dermatan & chondroitin sulphates • Affects predominantly Factor Xa. • Monitored with anti-Xa assay. Used only in ttt of HIT • Prolonged half-life in ESRD. • Danaparoid cross react with HIT antibodies (10%). But, fondaparinux does not. • Very expensive.

Thrombin inhibitors Hirudin, Argatroban & Melagatran • • Synthetic peptide derived from arginine. Metabolized in the liver. Direct thrombin inhibitors. Monitored by APTT. Huridin is no longer used. Argatroban is licensed for ttt of HIT. Very expensive.
 • Derived from leeches. • Forms complex with thrombin and inhibits")
Recombinant hirudin (lepirudin) • Derived from leeches. • Forms complex with thrombin and inhibits platelet aggregation. • Administered as a single bolus at the start of dialysis (0. 08– 0. 15 mg/kg). • Efective but expensive, and has a prolonged half-life (bleeding after repeated use). • Monitored by APTT (aiming 1. 5– 2. 5). Used only in ttt of HIT

Platelet inhibiting agents Epoprostenol & Nafamostat • Induces inhibition of platelet aggregation and vasodilatation. • Causes more clotting than full heparinization. • Hypotension, headache, flushing, nausea, vomiting, and chest and abdominal pain are possible side effects. • Very expensive.

Catheter Lock

Catheter Lock

Anticoagulants Which one to use ? • • IHD CRRT High risk of bleeding HIT

IHD • For patients without an increased bleeding risk or impaired coagulation and not already receiving effective systemic anticoagulation, we suggest: 5. 3. 2. 1: for anticoagulation in intermittent RRT, we recommend using either unfractionated or low-molecular-wieght heparin rather than other anticoagulations. (1 C)

CRRT • 5. 3. 2. 2: for anticoagulation in CRRT, we sugest using regional citrate anticoagulation rather than heparin in patient who do not have contraindications for citrate. (2 B) • 5. 3. 2. 3: for anticoagulation during CRRT, in patient who have contraindications for citrate, we sugest using either unfractionated or lowmolecular-weight heparin rather than other anticoagulations. (2 C)

High risk of bleeding • 5. 3. 3: For patients with an increased bleeding risk who are not receivig anticoagulations, we suggest the following anticoagulation during RRT: q 5. 3. 3. 1: we sugest using regional citrate anticoagulation rather than no anticoagulation, in patient without contraindications for citrate. (2 C) q 5. 3. 3. 2: we sugest avoiding regional heparinization during CRRT in patient with increased risk of bleeding. (2 C)

HIT
 q. Regional citrate anticoagulation. q. Heparin")
HIT • Treatment: ( Non heparin anticoagulation ) q. Regional citrate anticoagulation. q. Heparin free dialysis. q. Other alternatives: ü Heparinoids ( fondaparinux ) ü Direct anti-thrombin inhibitors

Problem solving Frequent clotting Clotting during dialysis • blood becomes very dark in circuit • streaking in dialyser • visible clots in bubble trap • visible clots in venous lines • clots in arterial end of dialyser (not just small strands) • venous pressure will drop if clot forming in dialyser, or rise if clot distal to monitor • arterial pressure may rise.

Problem solving Frequent clotting § Review priming: ü Heparin ü Air § Re-evaluat vascular access: ü Inadequate flow ü Interrupted flow § Re-evaluat heparinization: ü Small dose ü Delayed starting ü Failure of heparin pump

Problem solving Frequent bleeding • Evaluate vascular access • Evaluate needle insertion technique • Evaluate heparin dose

Thank you
- Slides: 52