What epidemiologic transition and social determinants of health


 • Described in the 1970 s (Omran, later Olshansky,")


 • Shift from a")
 and urbanization – Nutrition")







 • increased")
 Mathers et al 2003")
: decrease of mortality followed by decrease of fertility")


 China: 390 (1992) Thailand India")


 Decomposition of")



 Behaviors Physiological mechanisms")

 in response")





- Slides: 35
What epidemiologic transition and social determinants of health mean for developing and implementing NCD programs Pascal Bovet, MD, MPH University Institute of Social & Preventive Medicine, Lausanne Consultant for NCD, Ministry of Health, Seychelles WHO-IUMP International Seminar on the Public Health Aspects of NCDs Lausanne, 7 -12 March 2010
Outline • • Definition The four classical stages of the health transition The driving engines Demographic transition Epidemiological transition Global frameworks to model health trends Conclusion
The epidemiologic transition (health transition) • Described in the 1970 s (Omran, later Olshansky, Ault) – Relationship between socioeconomic development and health – Underlies shift from communicable diseases and nutritional deficiencies to NCDs – Classification of 4 stages to relate socioeconomic and disease patterns • Provides a framework to understanding current and future health patterns and needs – Particular relevance for developing countries experiencing early stages of health transition – Model for health planning, particularly where available data are scarce Omran AR. The epidemiologic transition: a key of the epidemiology of population change. Milbank Mem Fund Q 1971; 49: 509 -538 Olshansky & Ault. The fourth stage of epidemiologic transition: the age of delayed degenerative diseases. Milbank Mem Fund Q 1986; 64: 355 -91
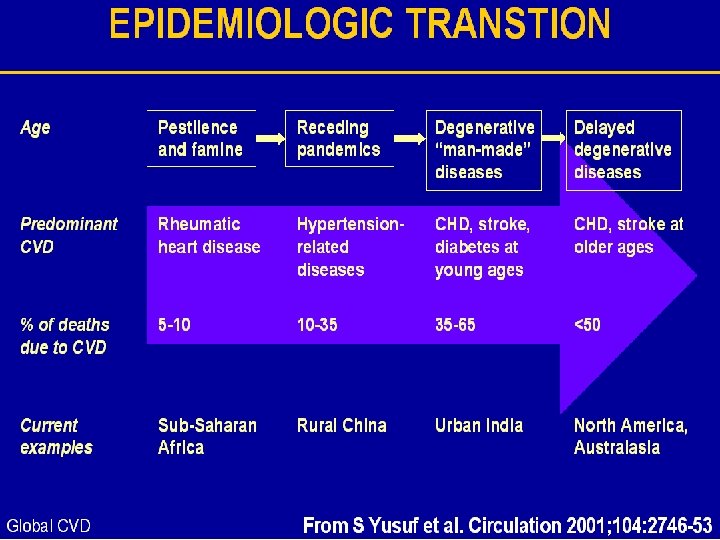
The 4 stages of the health transition Stages 1* 2* Socio. Life economic expecdevelopment tancy ~30 + Age of pestilence (LIC, rural SSA) (infection) and famine 30 -50 Age of receding++ (LIC-MIC) pandemics Main characteristics Broad disease categories (proportionate mortality) Infectious diseases CVD: 5 -10% of all † Nutritional deficiencies Related to nutrition/infection: RHD; cardiomyopathies) Improved sanitation : CVD: 10 -35% Hypertensive heart disease, infections, diet stroke, sequels of RHD (salt), aging 3* 50 -55 Age of degen. +++ and man-made (MIC, countries in transition) diseases aging, lifestyles related to high SES: sat fats, sugar, Inactivity, smoking) 4** Age of delayed ++++ degenerative (western countries) diseases risk behaviors CVD <50% (delayed stroke an IHD, CHD, aging population in the population (prevention and health & better treatment new promotion) and treatments >70 CVD: 35 -65% Obesity, dyslipidemias, HBP, ® IHD, stroke, often at early age Omran. The epidemiologic transition. Millbank Mem Fund Q 1971 ; 49 : 509 -38 Olshansky & Ault. The 4 th stage of the epidemiological transition. Millbank Mem Fund Q 1986 ; 64 : 355 -91
Main engines of health transition: demographic transition and epidemiologic transition Socioeconomic, public nutrition mortality economic social & sanitation ( infant mortality) development environment , housing, technology followed by Industrializat al changes health for health fertility ion & care urbanization wealth & per cap. + Heath care transition income, changes in environm. favoring adoption of increasi old risk behaviors NCD ng and persons at levels of RF: infectious aging risk of fat, calories, tobacco, diseases populatio developing sedentary habits ns NCDs
Changing socio-economic structures underlying adoption of unhealthy behaviors (nutrition transition) • Shift from a preindustrial agrarian economy to industrialization – Less active physical activity for individuals – Higher availability of cheap processed foods (high fat, high carb. ) • Profound changes in household technology (leads to less PA) – Food availability: canning, refrigeration, freezing, radiation, packaging – Food preparation: fossil fuels, electricity, appliances (cooker, mixers) • Dramatic shift in leisure activities for adults and children – Time spent for viewing television (sedentary habits) – Images/marketing brought to each household (alters consumption) Popkin B. The nutrition transition and obesity in the developing world. Nutr J 1991; 131: 871 -73
Globalization favors lifestyle transition • Trade liberalization (of world markets) and urbanization – Nutrition transition: fats, sugar (‘coca-colanisation’), ↓ complex carbohydrates – Supply larger than demand (large portions, “all you can eat”, etc), fuels competition & promotion, decreasing cost of $/calorie (fats, sugars): favors consumption – tobacco • Information & communication technologies – Global advertising & promotion of unhealthy lifestyles • Urbanization and accelerated migration of populations – Acculturation facilitates adoption of unhealthy lifestyles • CVD are transmitted diseases whose vectors are commercial & advertising practices
Epidemiologic transition: from traditional to modern nutrition
From traditional to modern food marketing. .
From ancient to modern work ….
From traditional to modern transportation. .
Village in Ghana, 2005
A model of the health transition accounting for mortality rates of diseases and broad cause of NCD
Emergence and decline of CVD: different stages of health transition along different development stages Rates of CVD:
Total mortality vs. age-adjusted mortality Aging populations: increasing NCD deaths (crude rates) • increased total burden & increased volume of HC • even if prevention programs are effective ≠ Epidemiological changes: age-adjusted mortality rates • age-adjusted NCD mortality can decrease even in LMIC • efficacy of programs/policy to be assessed by changes in age-standardized rates of NCD/risk factors
Share of DALYs by main causes and region (2002) Mathers et al 2003
Demographic transition (Mauritius, 1890 -1990): decrease of mortality followed by decrease of fertility
Demographic transition in Seychelles: NCD at age 50 -70 will inevitably increase by 3 -4 fold between 1990 and 2030
Developed Men 1960 Developing Women Demographic transition: major changes expected in LMIC 2000 2040 Note: “Population bonanza” before large proportion of population gets old (and large total NCD burden) Kinsella K & Wan H. U. S. An Aging World. Census Bureau, International Population Reports, P 95/09 -1: 2008. Washington, DC, 2009.
Epidemiological transition in LMIC: changes in cigarettes consumption (sales) China: 390 (1992) Thailand India UK US Department of Agriculture (1994)
Nutritional transition: rapid and generalized increase in consumption of fat, China Reddy &Yusuf. Circulation 1998; 97: 569
GDP & population levels of BMI, SBP, and cholesterol Ezzati E et al. Rethinking the ‘‘Diseases of Affluence’’ Paradigm: Global Patterns of Nutritional Risks in Relation to Economic Development. PLo. S 2005; 2; e 133
What will be driving NCD mortality in next 20 years? Deaths (millions) Decomposition of projected NCD into demographic and epidemiological components 2005– 2030 All chronic diseases Abegunde et al. Lancet, 2007 CVD & diabetes Cancer Respiratory diseases
Social determinants of health: relevance for NCD • Greatest share of health problems attributable to social conditions in which people live and work • Focus on “causes of the causes”, particularly relevant for NCD (“lifestyle”) • Highlights need for policies to protect health across all sectors (“health in all policies”) • Effective policy to address health challenges must tackle underlying social conditions that make disadvantaged people more vulnerable The Final Report of the WHO Commission on Social Determinants of Health. 28 August 2008
Framework of the major categories and pathways of determinants of health inequities and well-being WHO Commission on Social Determinants of Health, August 28 2008
Interaction between heath transition & social determinants on the occurrence of NCD Conditioning/modifying factors: poverty, education, stress, SDH Globalization Urbanization Diet Environment & lifestyle changes Physical activity Tobacco Blood pressure Cholesterol Obesity Diabetes Mortality & Morbidity
Social inequalities Fundamental intervention 1. Reduce social inequality Stress (“Ideological” orientation) Behaviors Physiological mechanisms Mechanistic intervention 2. Reduce the main risk factors population wide Social inequality in CVD From Davey Smith (“Pragmatic” public health orientation)
Hypothesized effects of different interventions to reduce social inequalities in CHD – which is more “effective”? CHD Rate / 100 K ORIGINAL SOCIAL INEQUALITY IN CHD 1 2 1. “Make the poor like the rich”, so they would have the same CHD levels as the rich 2. Intervene to substantially reduce the main risk factors regardless of social group Social Disadvantage From Davey Smith Social Advantage
Transition from traditional to modern risks can vary largely (negative or positive) in response to enforced policies Global health risks: mortality and burden of disease attributable to selected major risks. WHO 2009
Gapminder www
Response to the health transition POPULATIONS Demographic and social determinants High Risk Low Risk Public health interventions (upstream: policies that shape the economic, social and physical environments to facilitate and enable healthy behaviors) INDIVIDUALS Low Risk Biology + beliefs + behaviors High Risk Clinical + behavioral interventions (downstream: policies that support health services and clinical interventions)
The health transition in developing countries: conclusions • Link between demographic/social changes and disease patterns • Need to address broad causes of diseases (SD, etc) • Transition to NCD results from success in controlling infectious diseases • Build on experience gained on control of infectious diseases • Transition to NCD is inevitable as populations are aging • Allocate resources: tsunami of NCD it is going to happen • Double burden of diseases in many countries • Plan strategically, effectively and globally • Don’t forget that there nothing more practical than a good theory !! • Transition model provides basis for prospective planning, also when current epidemiological data are not available locally • Good news: last transition stage predicts improved health in populations conditional to appropriate policy and health care response
Policy framework for NCD prevention and control (to speed transition to optimal health stage in populations) Reducing energy intake, incr. PA, red. smoking, etc Adapted from: Sacks et al. Obes Rev 2008 (from WHO Global Strategy on Diet, PA and Health: a Framework to monitor and evaluate implementation)
Health transition: a tool for anticipating and planning health response ! I skate where the puck will be Wayne Gretsky « Greatest hockey player of all time »