TISSUE DOPPLER IMAGING DR PRASANTH S Introduction TDI









 J Am Soc Echo 2001; 14: 1143")

















 with Tissue Doppler Imaging (TDI)")









 middle transverse layer. 2) inner oblique layer(descending segment)")









- Slides: 63
TISSUE DOPPLER IMAGING DR PRASANTH S
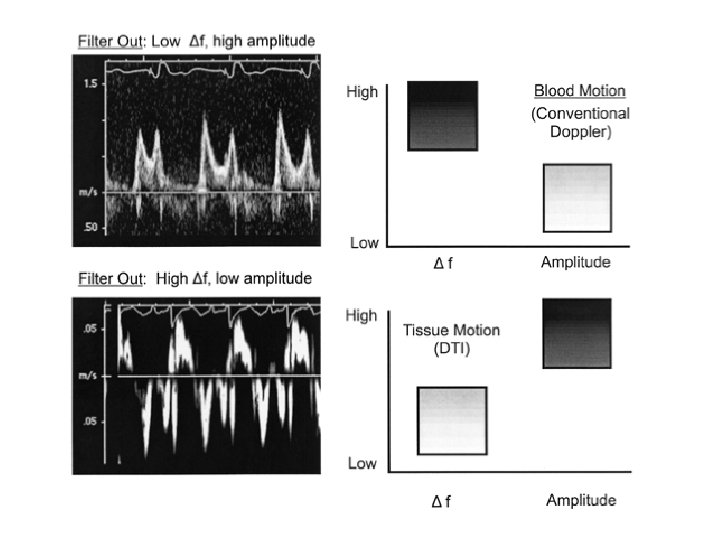
Introduction • TDI uses Doppler shift data from the myocardium to obtain qualitative and quantitative information on myocardial wall motion. • Measures the velocity of myocardial wall motion v. Low velocity • 5 to 20 cm/s • 10 times slower than velocity of blood flow v. High amplitude • Approximately 40 decibels higher than blood flow Int. J of Card Imaging 2001; 17: : 8
Doppler tissue Vs blood pool imaging
Tissue Doppler –imaging modes – Pulse wave Doppler – Color 2 D imaging – Color M- Mode
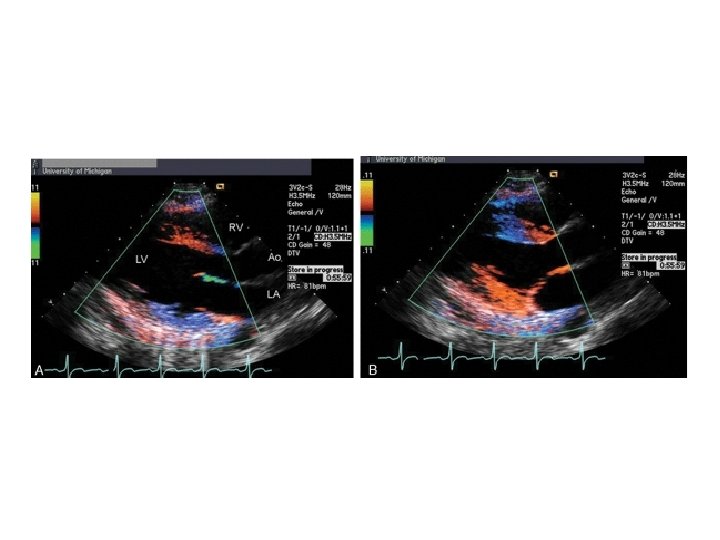
2 D Colour TDI • Colour-coded representation of myocardial velocities- superimposed on gray-scale 2 dimensional images. • indicate the direction and velocity of myocardial motion. • increased spatial resolution and the ability to evaluate multiple structures and segments in a single view.
M-mode colour Doppler tissue imaging • Colour-encoded images of tissue motion along an M-mode interrogation line. • High temporal and spatial resolution.
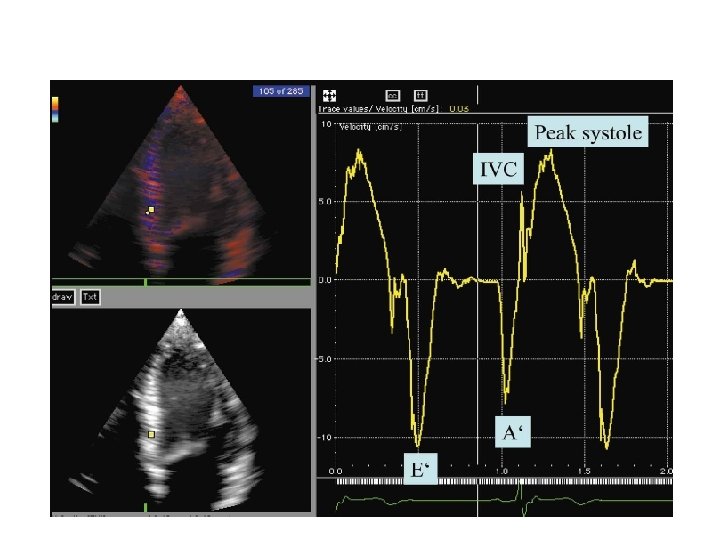
Pulsed-wave TDI • Used to measure peak myocardial velocities • Mitral annular motion: Good surrogate measure of overall longitudinal left ventricular contraction and relaxation. • To measure longitudinal myocardial velocities, the sample volume is placed in the ventricular myocardium immediately adjacent to the mitral annulus
Pulse Wave Tissue Doppler
Diastolic components of myocardial velocities correlate with mitral inflow velocities
Normal Myocardial Velocities : Basal Segments (cm/s) J Am Soc Echo 2001; 14: 1143 -52
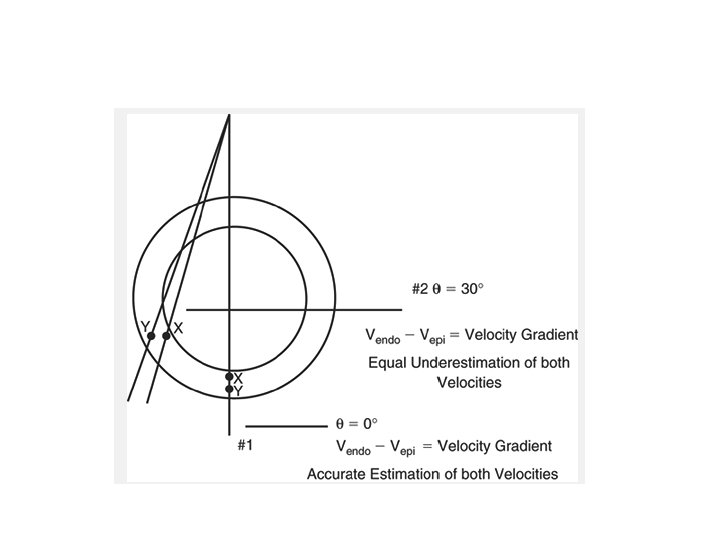
Myocardial Velocity Gradient • Difference in myocardial velocity between the endocardium and epicardium divided by the myocardial wall thickness • Reflects rate of change in wall thickness • MVG is an indicator of regional myocardial contraction. • Determined in a single segment with the same angle of interrogation of the Doppler beamrelatively angle independent J Am Coll. Card 1995; 26: 217 -23
CLINICAL APPLICATIONS OF TDI
Assessment of LV Systolic Function • Sa- Correlated with LV ejection fraction. • Peak systolic velocities were measured at 4 different sites of the mitral annulus. • A cut-off point of ≥ 7. 5 cm/s had a sensitivity of 79 % and a specificity of 88 % in predicting preserved systolic function or ejection fraction of ≥ 0. 50. • Regional reductions in Sa - regional wall motion abnormalities. J Clin Basic Cardiol 2002; 5: 127
Regional Systolic Function • Pulse wave tissue Doppler after anteroseptal MI. • Decreased velocity in the septum (top). • Normal velocity in the lateral wall (bottom).
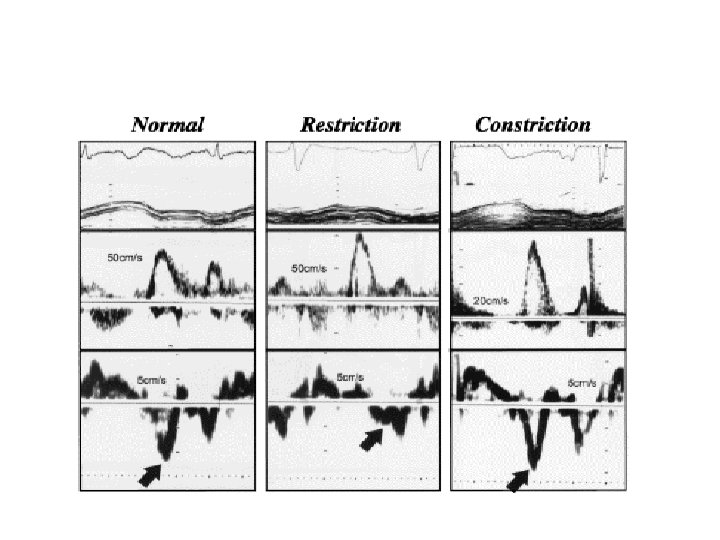
Diastolic Dysfunction Impaired relaxation Pseudonormal Restrictive
• Transmitral flow velocities are dependent on LA filling pressures. • Psuedonormalization occurs as LA pressure increases. • Difficult to diagnose diastolic dysfunction from mitral flow velocities. • Myocardial velocities are persistently reduced in all stages of diastolic dysfunction. • TDI assessment of diastolic function is less preload dependent.
Diastolic Dysfunction NORMAL Impaired Relaxation Pseudonormal Restrictive Filling DT <220 ms >220 ms 150 -200 ms <150 E/A 1 -2 <1 1 -2 >2 Em >8 <8 <8 <8
Diastolic Dysfunction
Estimation of LV Filling Pressures • LV filling pressures are correlated with the ratio of the mitral inflow E wave to the tissue Doppler Ea wave (E/E’) • E/lateral E’ ≥ 20 - elevated LV end-diastolic pressure. • E/E’ = 5 -15 is correlated with a normal LV EDP • E/E’ > 20 predicted PCWP > 15 mm of Hg with 92% sensitivity and 82% specificity Nagueh et al
Constrictive Vs Restrictive Physiology • Constrictive pericarditis with normal LV function have normal or elevated Em velocities. • Doppler Em velocity of 8 cm/s differentiates constriction and restriction. • Restrictive < 8 cm/s • Constrictive > 8 cm/s
Assessment of Right Ventricular Function • Important prognostic indicator in patients with heart failure and in postinfarction patients • Reduced tricuspid annular velocities with TDI have been documented in Post inferior myocardial infarction, chronic pulmonary hypertension, and chronic heart failure.
Limitations • Accuracy of velocities dependent on angle of ultrasound beam. • Not all wall velocity obtainable from every view. • Wide range of normal values. • Even non contractile myocardium will be pulled by near by segments resulting in apparent velocity component.
Strain Rate Imaging
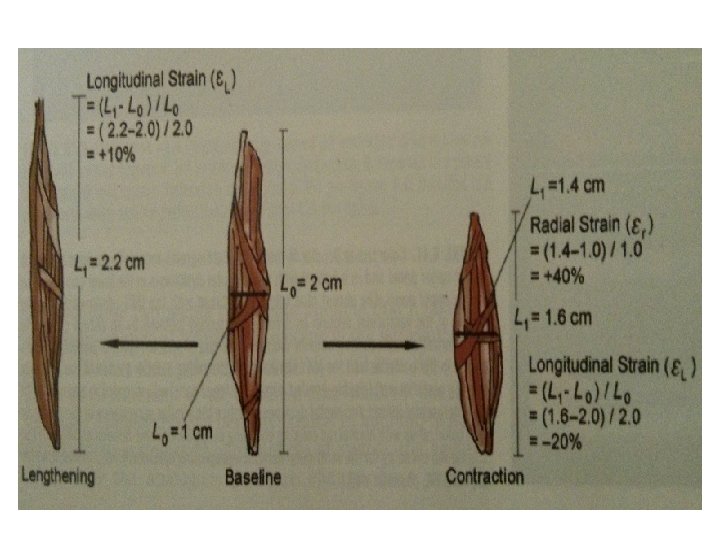
Introduction • Evaluation of a myocardial region with reference to an adjacent myocardial segment. • Deformation analysis- analysis of ventricular mechanics or shapes during cardiac cycle. • Myocardial strain, strain rate, torsion. • Strain- percentage thickening or deformation of the myocardium during the cardiac cycle. • Change of strain per unit of time is referred to as strain rate
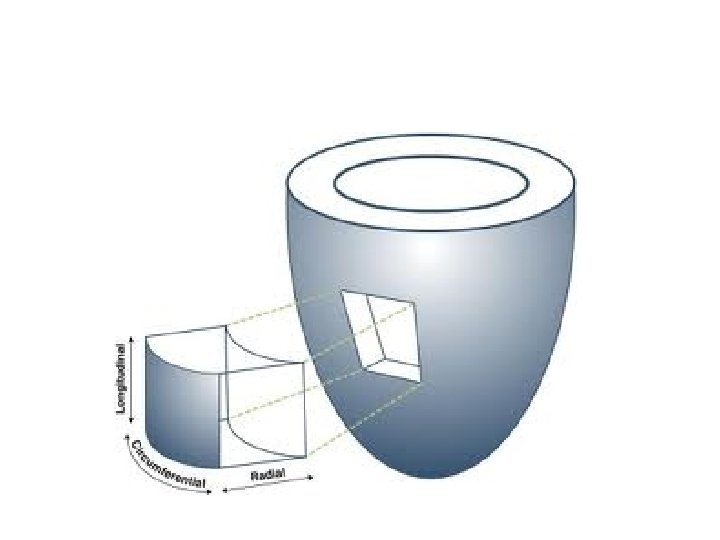
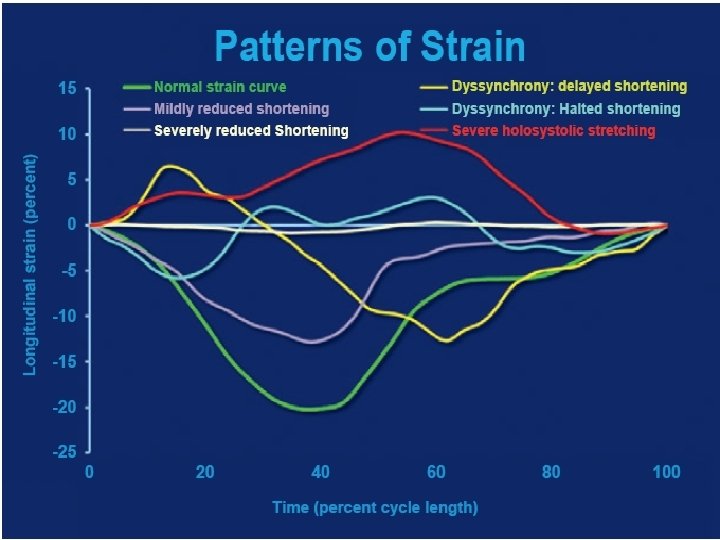
• Strain calculated in three orthogonal planesrepresenting longitudinal, radial, circumferential contraction. • Negative strain- shortening of segment. • Positive strain- lengthening of segment
Strain & Strain rate
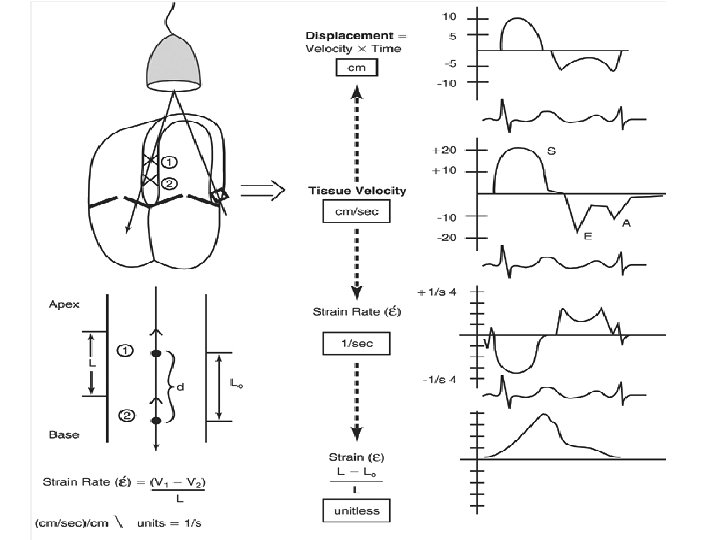
Methods Doppler tissue imaging • Two discrete points are compared for change in velocity • Strain rate- primary parameter obtained • Strain –derived by integrating velocity over time. Speckle tracking • Actual location of discrete myocardial segments calculated. • Strain is the primary parameter. • Strain rate-derived by calculating change in distance over time.
Comparison of Two-Dimensional Speckle Tracking Echocardiography (2 D STE) with Tissue Doppler Imaging (TDI) 2 D STE TDI Deformation analysis in 2 dimensions. One-Dimension measurements Angle independent Measurement dependent on angle Better spatial resolution Limited spatial resolution Less time-consuming data acquisition and easy data processing. Time-consuming Lower temporal resolution High temporal resolution Dependent on high resolution image quality Image quality less important Lower interobserver variability Higher interobserver variability Lower optimal frame rate limits the reliability of measurements in patients with tachycardia
SR- Doppler tissue imaging
Speckle tracking • ‘Speckles’ are small dots or groups of myocardial pixels that are created by the interaction of ultrasonic beams and the myocardium. • Considered as acoustic fingerprint for that region. • This enables to judge the direction of movement, the speed of such movement, and the distance of such movement of any points in the myocardium.
Speckle
Method • Track the endocardial and epicardial borders of the left ventricle • Correctly define the region of interest (ROI) in the long or short axis view • Post-processing software automatically divides the ventricle into six equally distributed segments • 2 D or 3 D data set is produced • Mathematical algorithms are applied to generate values
• Strain is not uniform among all myocardial segments. • Radial strain-Magnitude of basal parameters are higher than the apical values. • Longitudinal strain- less variability fron apex to base. • Circumferential strain- higher in anterior and lateral walls compared to posterior and septal. • Normal longitudinal strain averages -20% • Normal radial strain about +40%
Normal Strain Displays Wave Forms , Curved M-mode
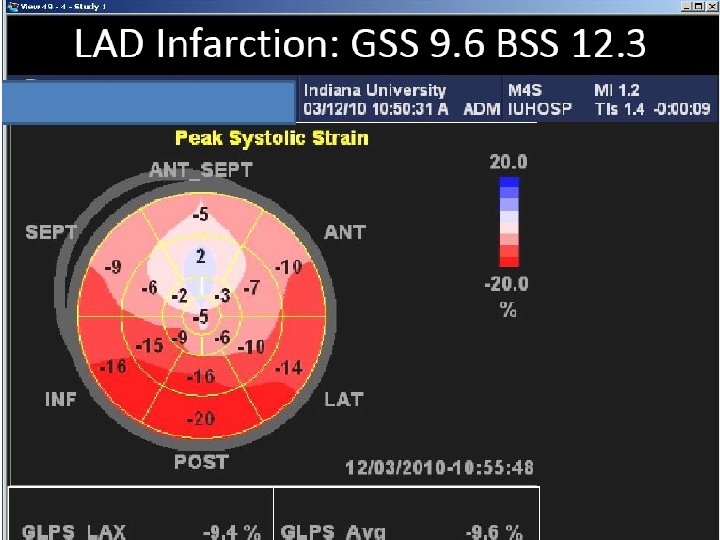
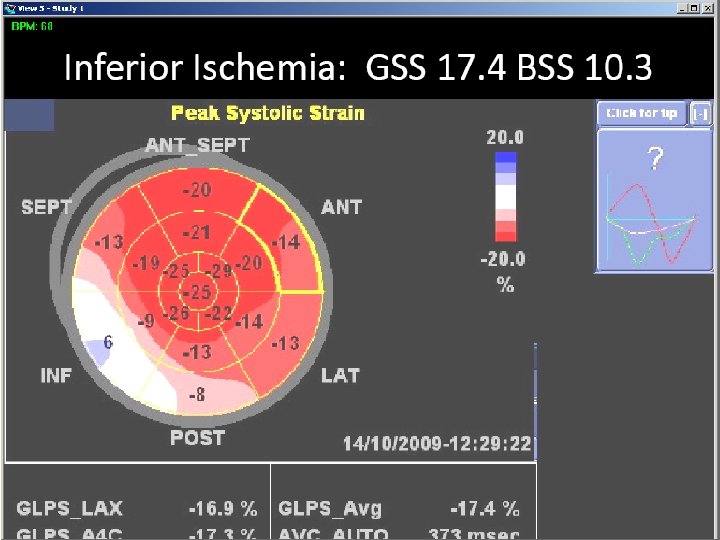
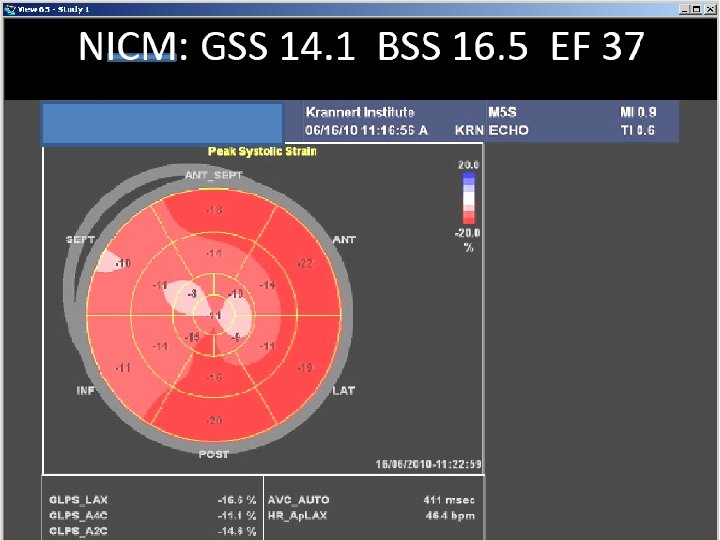
Normal Strain Displays- bulls eye presentation
Normal pattern Dilated cardiomyopathy Dyssynchrony
Velocity vector imaging
Cardiac muscle • 3 layers 1) middle transverse layer. 2) inner oblique layer(descending segment) 3) outer oblique layer( ascending segment)
VENTRICULAR TORSION • Similar to the winding and Unwinding of a towel. • Isovolumetric contraction -the apex and base rotates in counterclockwise direction. • Ejection phase apex rotates counterclockwise & base rotates clockwise when viewed from the apex • Diastole - relaxation of myocardial fibres - recoiling clockwise apical rotation. • Isovolumetric relaxation- both apex and base rotates in clockwise direction.
Myocardial mechanics
• Rotation - Measure of the rotational movement of the myocardium in relation to an imaginary long axis line from apex to base drawn through the middle of LV cavity. • Twist (degrees) is the net difference between apical and basal rotation • Torsion - Twist divided by the vertical distance between the apex and base and is expressed as degrees/cm.
VENTRICULAR TORSION
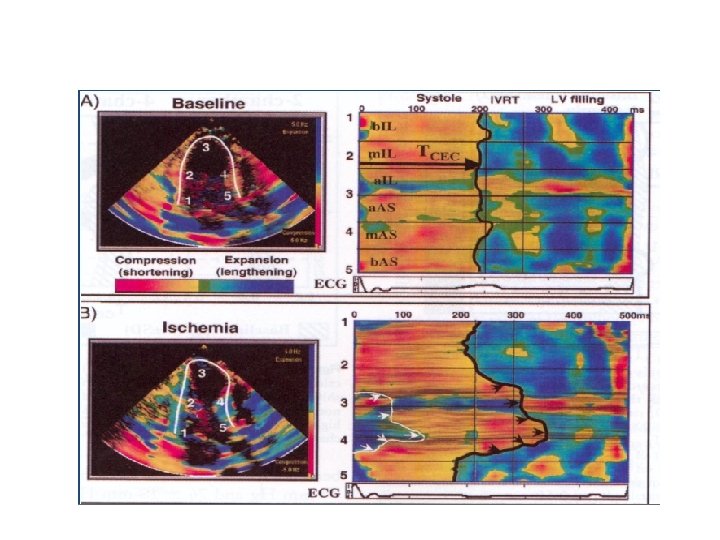
CAD- Myocardial ischemia, Myocardial infarction, Myocardial viability • Reduction in strain by 2 D STE more objective and accurate than the traditional visual method of assessing WMA. • Post systolic thickening (deformation)by radial strain correlates with the severity of ischemia. • To differentiate transmural from subendocardial infarction- lower circumferential strain in the former
Applications • Heart failure with normal LVEF Reduced and delayed LV untwisting—at rest and exercise • Cardiac resynchronization therapy (CRT) Speckle Tracking and Resynchronization (STAR) study showed radial and transversal strain better than longitudinal and circumferential strain in predicting LVEF response and long term survival after CRT. Lack of dyssynchrony before CRT by 2 D STE radial strain associated with death or hospitalization for heart failure
Twist in DCM Am J Cardiol 2008; 101: 1163– 1169, 2008
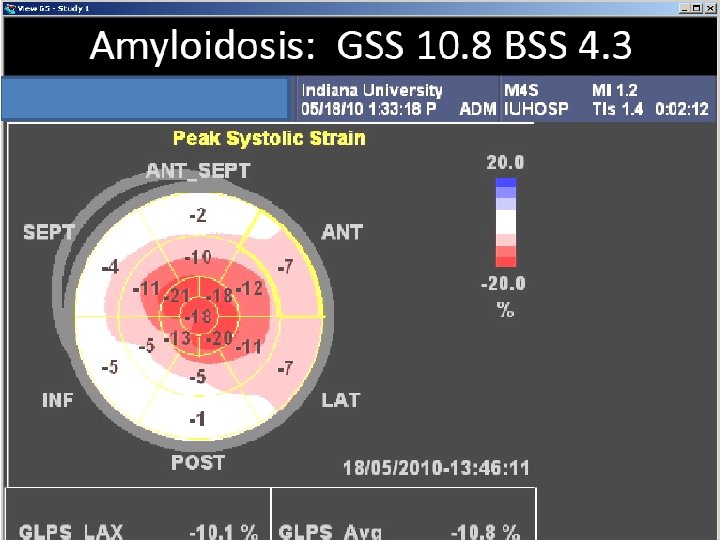
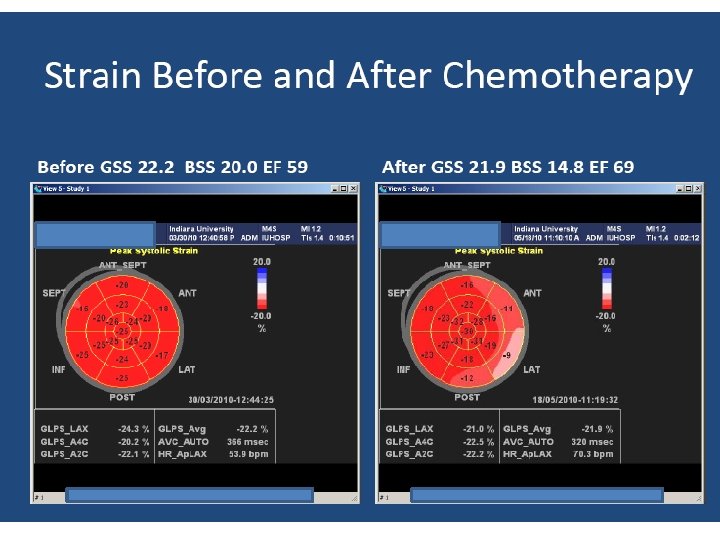
Applications • Stress cardiomyopathy. • Restrictive cardiomyopathy. • Detection of subclinical diseases/early myocardial involvement. • Detection of rejection and coronary stenosis in heart transplant patients. • Early detection of chemotherapy induced cardiotoxicity. • Valvular heart disease. Decreased radial, circumferential and longitudinal strain in patients with severe aortic stenosis and normal LVEF. Long term follow up after valve replacement showed significant improvement in strain.
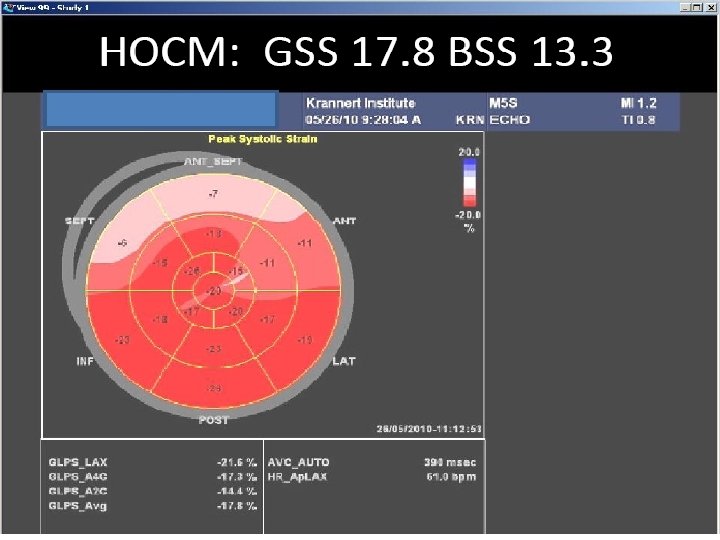
Differentiation of Athlete’s Heart from Hypertrophic Cardiomyopathy Athlete’s Heart Hypertrophic Cardiomyopathy Normal longitudinal and other types of strain Decreased longitudinal strain Increased LVEDV Decreases after deconditioning for 3 months. Decreased LVEDV No change with deconditioning. Increased LV twist. Delayed LV untwisting. Increased early LA strain rate. Reduced LA strain and strain rate