Southern Health Medical Conference 2013 Sue Harriman Acting


































 Peter Hockey")

 is a simple and short 30 item survey instrument consisting of ten")













- Slides: 59
Southern Health Medical Conference 2013 Sue Harriman Acting Chief Executive 10 -11 July 2013
Our aim is to provide high quality safe services which improve the health, wellbeing and independence of the people we serve. We have set ourselves three stretching goals which guide our strategy and are the basis on which we measure our performance as an organisation.
Our integrated service portfolio Integrated Service Divisions We provide community services for adults & older people, organised into 4 localities aligned to CCGs. Over the last 6 months we integrated our physical health & older people’s mental health services and are pursuing strategies of greater integration with primary, acute and social care Specialist Mental Health services We provide specialist mental health services including Adult Mental Health – where our focus is on delivering recovery orientated services and redesigning care pathways resulting in more care provided in community settings – and specialist secure services for adults and young people Learning disability services We provide specialist support to adults with learning disabilities in the community and in our inpatient services. Following a merger with Oxford Learning Disability NHS Trust in 2012, we now deliver care across Hampshire, Oxfordshire, Buckinghamshire, Wiltshire, Dorset and Swindon. Social care services Through our social care division, TQTwentyone, we provide social care services for people with learning disabilities or mental health needs in Hampshire, Oxfordshire, Swindon and Dorset, for older people leaving inpatient services in Hampshire and for children with a learning disability Children’s Services Through teams of health visitors & school nurses we provide public health services for children and families, and provide speech and language therapy, physiotherapy and occupational therapy. Children’s services work increasingly closely with Hampshire County Council.
Our principles INTERNAL REDESIGN Doing everything we can internally to redesign our services to provide better quality & better value for money GROWTH Growing our business where this means we can deliver better outcomes, better patient experience or be more efficient INTEGRATION Working with our partners to develop an integrated health and social care system
Our approach to quality Patient Safety Clinical Outcomes Patient Experience Continuous Improvement Our Quality Strategy is framed around the three domains of safety, experience and outcomes, with an overarching driver of continuous improvement.
The core themes of our workforce strategy 1. Developing our leadership capacity and capability, so that we create the culture and behaviours we need to improve our services and deliver our vision 2. Designing and developing our workforce so that we have productive people with the skills, competencies, information and contractual arrangements we need 3. Improving how we engage with our workforce so that they are motivated to do the best they can for our patients, customers and for Southern Health
The core themes of our financial strategy Building on our current financial strength, targeting investment to modern services and technology CIP delivery based on service redesign with savings delivered from transformation. £ 18. 3 M CIP plan for 2013/14 Refresh of our Estate Strategy in light of the Transfer of Community Services Influence of national policy on future financial plans Looking for opportunities in emerging markets, managing threats in our existing markets
Southern Health Medical Conference 2013 Dr Helen Mc. Cormack Chief Medical Officer 10 -11 July 2013
The people behind the stories …
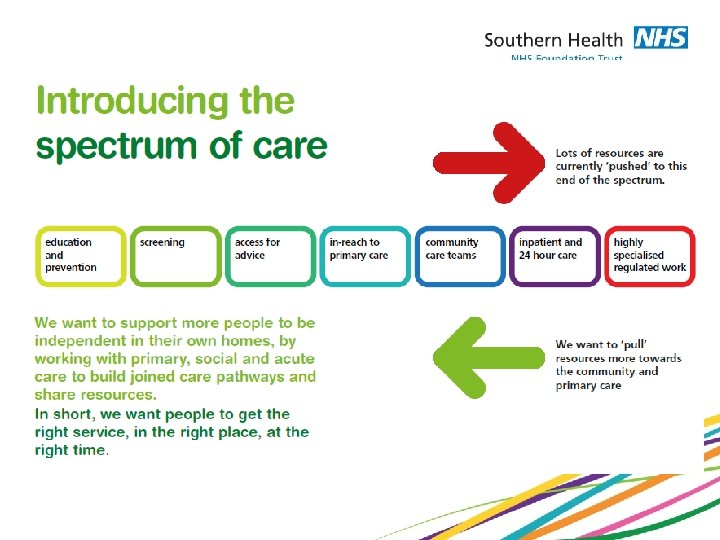
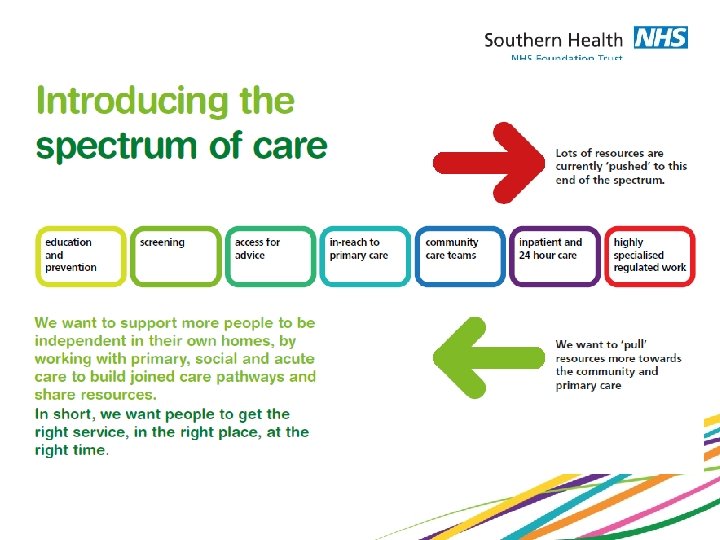
Lots of time and energy are currently “pushed” to this end of the spectrum having a satisfying and meaningful life opportunity; for yourself and for getting involved agency; gaining a sense of self control We want to support self determination, self management and partnership working to achieve excellence for our patients and our working lives hope; the possibility of a future and a sense of purpose education and training; gaining the skills you need delivery of priority improvements; policy, procedure and guidance highly regulated systems; external scrutiny and inspection We want to “pull” our resources and focus our attention to this end of the spectrum
The people behind the stories …
Southern Health Medical Conference 2013 Jo Hennessy & Sarah Law Talent Works Ltd
Mid-Staffordshire Trust failed to tackle an insidious negative culture involving a tolerance of poor standards and a disengagement from managerial and leadership responsibilities. The Francis Report Doctors have a long tradition of using will and determination to solve complex problems. If doctors could be encouraged to see “the system” in the same way they see a patient, success in healing the healthcare system would seem ensured. Reconstructing Medical Practice, C Jorm
Aims of the conference Align and enhance the relationship between doctors, the senior management team and the wider organisation Provide a genuine opportunity to shape and influence both the current situation and future organisation, given the Francis Report as a key driver Enable everyone to feel more valued and engaged
How engaged are you right now? Many definitions of engagement Themes around thinking, feeling and acting positively; likely to go the extra mile Not at all Engaged Fully Engaged 1 2 3 4 5 6 7 8 9 10
Conference Day One Divergent thinking Mixed groups of people Exploratory conversations Generates questions, ideas, challenges Could be stimulating; could be frustrating!
Conference Day Two Focussed thinking Real work teams “So what? ” conversations Steal ideas with pride Creation of action plans
Conference process - today Three discussion starters – Duty of Candour – Patient Safety – Inter-professional working Table work – Sharing experiences Collective outputs – – How is it right now? How do we want it to be? What is working now that should continue? Ideas and questions to be explored further
Introductions Who you are, what you do, where you do it… What your hopes are for this conference Suggestions for Ground Rules
Inter professional working How is it right now? How do we want it to be? What is working now that should continue? Ideas/questions to be explored further
Patient Safety - How do we want it to be ?
Linking discussions to our reality Opportunity to reflect and make sense of the day Find a partner from another table Consider potential links and challenges between Duty of Candour, Patient Safety and Inter. Professional Working What has irked you today? So what? What has inspired you today? So what?
Welcome to Day Two Please sit with your team
Reconnection The best bit for me yesterday was… Something I would like to talk about more today
Conference process today The future of clinical leadership – Peter Lees Our Medical Compact – Jude Diggins & Peter Hockey Turning ideas into action - you Sharing our commitments – you again Closing thoughts – Helen Mc. Cormack and Peter Hockey
Working on our Medical Staff Compact Peter Hockey & Jude Diggins
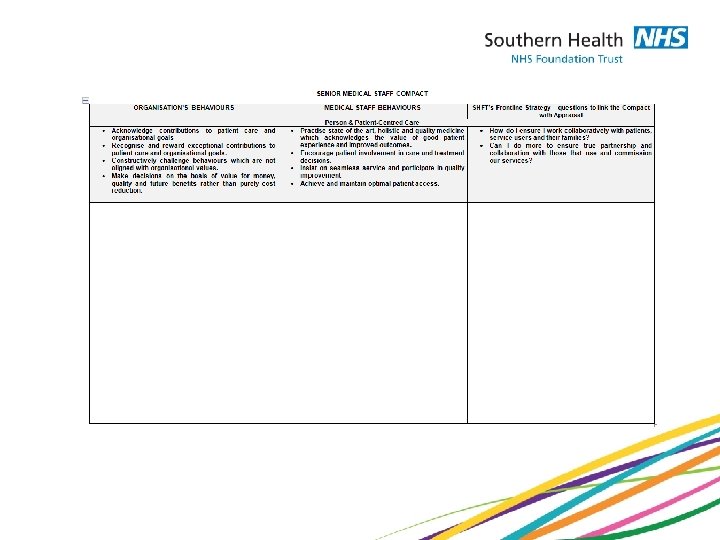
What is a Medical Staff Compact? • A compact is an agreement that clearly states the commitment of the medical staff and organisational leadership to one another for the purpose of improving patient care and meeting the aspirations of the organisation and its staff • It is developed by the medical staff and organsiational leadership as a “living” document to help achieve a shared vision. The compact will evolve as healthcare changes.
The compact means that Medical Staff and SHFT leadership will work together to achieve: • Better coordinated care and services for doctors and patients • Improved patient outcomes • Ease of access to key patient information • Improved services that will result in a sustainable organisation
Development of the Compact to date • A ‘good idea’ supported by SLT • Based on VMMC compact and SHFT agreed behaviours • Shared with CMO and CDs • Then shared with Executive Team • The compact is not done – we are seeking input from our medical staff • Will show some congruency with the Frontline Strategy
Leadership is key Leaders can drive cultural shift an change The world and those in it must be viewed holistically Staff and patient well being must be our focus
The strategy We must be clear about what we expect We must respond to negativity about the care we provide Everyone needs to sign up It is up to you how we do it
The ask from us now: - • Each table has a part of the compact • Please write comments/suggestions on the A 3 paper • Consider whether this is for medical staff only • We will collate and revise the compact based on suggestions
Turning ideas into action Your opportunity to really work on your service, for your patients, with your team
Sharing our commitments One minute only! ONE Choose action that we commit to as a team…….
Medical Engagement (part 2) Peter Hockey
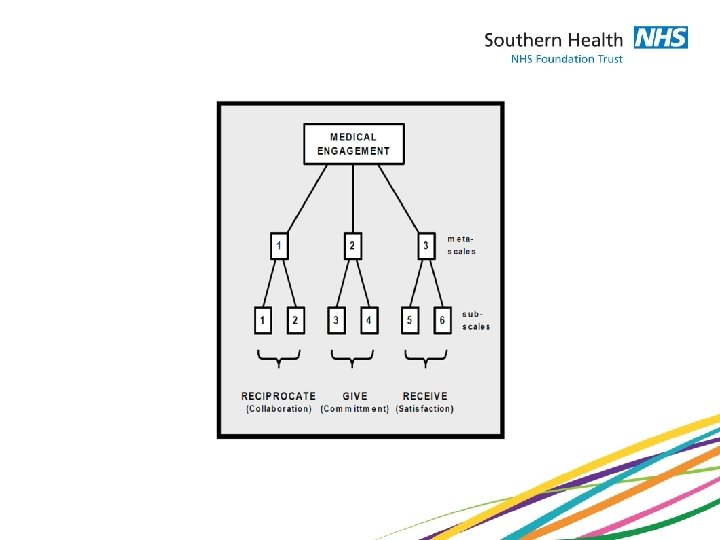
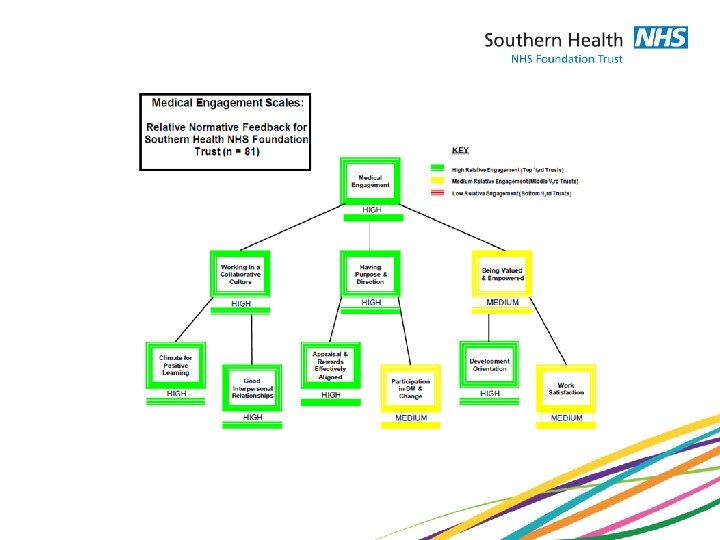
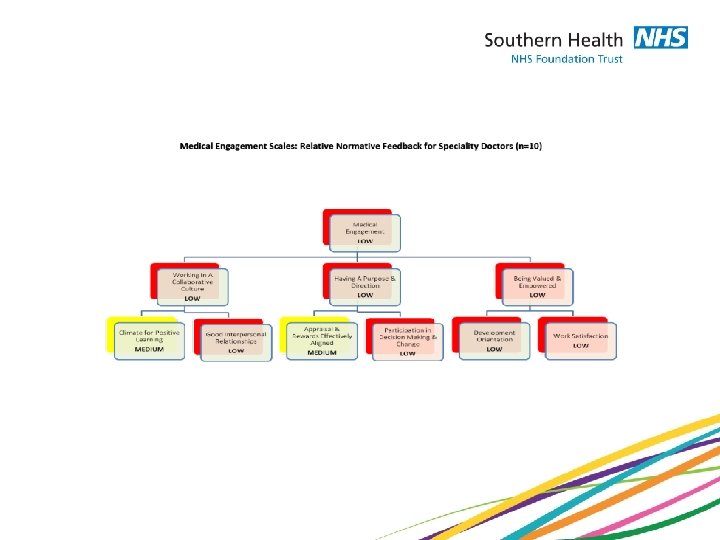
(MES) is a simple and short 30 item survey instrument consisting of ten reliable and valid scales. The instrument has a hierarchical structure and provides an overall index of medical engagement together with an engagement score on three reliable meta-scales with each of these three meta-scales itself comprising two reliable sub-scales: Meta-Scale 1: Working in a collaborative culture Sub-Scale 1: Climate for positive learning Sub-Scale 2: Good interpersonal relationships Meta-Scale 2: Having purpose and direction Sub-Scale 3: Appraisal and rewards effectively aligned Sub-Scale 4: Participation in decision-making and change Meta-Scale 3: Feeling valued and empowered Sub-Scale 5: Development orientation Sub-Scale 6: Work satisfaction
Furthermore, the structure of the MES enables it to contain two types of engagement sub-scale: - Three ORGANISATIONAL Sub-Scales (1, 3 and 5) which reflect the cultural conditions which facilitate or inhibit medical staff to be more actively involved in leadership and management Three INDIVIDUAL Sub-Scales (2, 4 and 6) which reflect medical empowerment and confidence to tackle new management and leadership challenges
Key Messages • Medical Workforce are more engaged than we thought • A few ‘nay-sayers’ can have a very negative effect • Our medical leaders are highly engaged • We have identified areas where we need to go from ‘Good to Great’ • Let’s capitalise on the positives and think about what else we want from our medical workforce
The ‘real value’ came from free text comments • ‘Lack of appreciation, valuing of medical expertise, knowledge and professionalism’ • ‘The increasing scrutiny in appraisal, revalidation, job planning’ • ‘Could there be some sort of very easy to use directory on the website so you can quickly find what you're looking for? ’ • ‘In spite of the cost of consultants, the perception is that engagement and development excludes the majority of doctors’ • ‘There is a view that the voice of doctors, and consultants in particular is not listened to, or comments valued’ • ‘The biggest risk at the current time is that consultants are so peeved, disappointed and disengaged that they throw the baby out with the bath water by refusing to have anything to do with organisational and corporate development. That will, more than anything else, really disempower consultants as a group of professionals’
You said, we did
Medical Advisory Committee • Overwhelming desire to keep and revamp • New Terms of Reference • Elections soon • Reporting into Clinical Advisory Forum • More focus on education, research, innovation and humanity!
Senior Medical Staff Committee • Great support to retain this forum • Not a Trust Management committee • Important forum to link whole staff with CEO and Executive Team • Meet twice a year • Should this conference be one of them?
How would you like us to ‘measure’ engagement?
5 minutes on each table to discuss the 3 S’s of Engagement - What would Service Users be saying? - What would Staff be saying? - What would Stakeholders be saying? - Feedback from each table - Aim to report back next year
Sharing our commitments One minute only! One thing we commit to as a team…….
Sharing our commitments A key learning for us as a team from this conference… An important first step we will be taking… How we are going to ensure this really happens…
Frequency Engagement Day One - includes Senior Managers Level of engagement
Engagement Day One - excludes Senior Managers
The three S’s of engagement If we had a fully engaged medical community… What would service users be saying? What would staff be saying? What would stakeholders be saying?