Single Ventricle Physiology with Pulmonary Hypertension Decisions and












")
 Shunt Revision 1")


 (*P=0. 000) SCMC data")
 (*P=0. 000) SCMC data")



- Slides: 22
Single Ventricle Physiology with Pulmonary Hypertension: Decisions and Challenges Xinwei Du M. D. Shanghai Children’s Medical Center
Single Ventricle Physiology • With restrictive pulmonary blood flow • With neither restrictive pulmonary nor systemic blood flow • W/O restrictive pulmonary blood flow but with restrictive systemic blood flow
Single Ventricle Physiology Normal Heart Fontan
PVR • Success of Fontan operation depends on lower PVR • Even slight increases in PVR sig. reduce the transpulmonary blood flow → failing Fontan • Pulmonary arteries • Pulmonary vascular bed • Pulmonary venous return • Atrial septum
Surgical Techniques in Stage I Palliation • PA Banding • DKS or Norwood • Palliative Switch
PA Banding • Must have an obstructionfree SVOT anatomy R. A. Jonas
Why do DKS? Increasing restriction at BVF Obstruction to systemic outlet Decreased ventricular compliance R. A. Jonas <2 cm 2/m 2
DKS • DHCA or DHLF • Source of pulmonary flow can be a B-T or Sano shunt
Lesions with Obstruction at BVF • DILV with discordant ventriculoarterial connection • TA with discordant ventriculoarterial connection • DORV with MA
PAB+APW The distance between the pulmonary valve to the bifurcation should be long enough for AP window creation
Palliative Switch l Coronary pattern should be Yacoub A l Aortic-pulmonary position should be anterior-posterior l Aortic root should not be too small
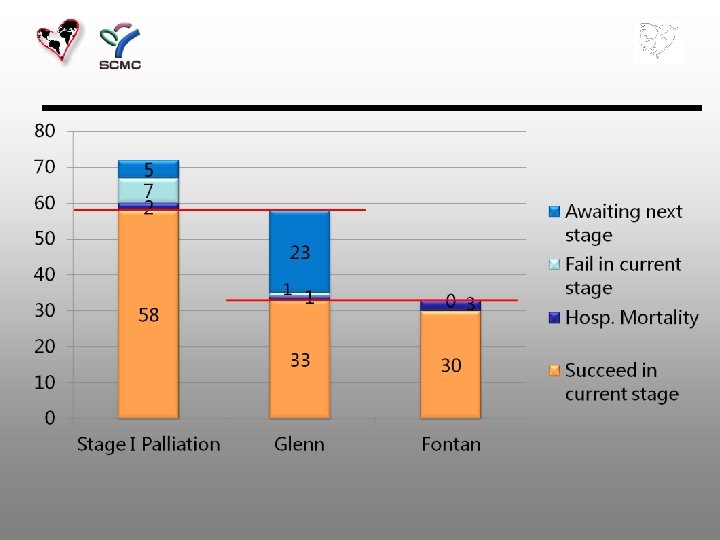
SCMC Data • 2002. 1 – 2014. 12 • 72 patients
Stage I Palliation Hospital Motality = 2. 8% (2/72)
Re-operation before Stage II Glenn Rebanding 5 8. 4% (5/59 ) Shunt Revision 1 7. 6 (1/13) Other (Bleeding, Chylothorax) 2
9 Patients Failed at stage I Palliation n 2 hospital motality n 7 fail to pursue Glenn • Present late (after 6 m) • Post-op. AV valve regurgitation • Heterotaxy • m. PAP > 25 mm. Hg 5 4 5 6
Pulmonary Vasodilator after Fontan • PVRI > 3. 0 Wood units. m 2 • m. PAP > 15 mm. Hg • CVP > 20 mm. Hg • TPG > 10 mm. Hg • Desaturation • Persistent PE
Iloprost therapy after Fontan Effect iloprost on TPG (mm. Hg) (*P=0. 000) SCMC data TPG 1: Before iloprost (14. 5 ± 2. 7) TPG 2: Before extubation (9. 5± 2. 3) TPG 3: After extubation 30 min later (8. 1± 1. 9)
Iloprost therapy after Fontan Effect iloprost on CVP (mm. Hg) (*P=0. 000) SCMC data CVP 1: Before iloprost (19. 8 ± 5. 2) CVP 2: Before extubation (12. 4 ± 2. 6) CVP 3: After extubation 30 min later (11. 4 ± 2. 4)
Oral Bosentan after Fontan • 40 patients • 6 months follow-up
Conclusion • Stage I palliation is the key point to treat single ventricle physiology with unrestricted pulmonary blood flow • Early diagnosis ensure a good long term outcome • Pulmonary vasodilators help to improve cardiac performance in patients with high PVR postoperatively
Thank you !