PSYCHOLOGY Chapter 15 PSYCHOLOGICAL DISORDERS Power Point Image






















 Repetitive hand washing and (b) checking (e. g. , that")


































- Slides: 58
PSYCHOLOGY Chapter 15 PSYCHOLOGICAL DISORDERS Power. Point Image Slideshow
CHAPTER PRETEST • What are Mental Disorders? • How are Mental Disorders Defined, Assessed, and Diagnosed? • What are Anxiety Disorders? • What are Mood Disorders? • What are Schizophrenia Spectrum and other Psychotic Disorders?
CHAPTER TOPICS • Some Final Thoughts: Syndromes without Stigma? • Summary
PSYCHOPATHOLOGY q. Psychopathology is defined as the study of mental illness or mental distress. This definition also includes the manifestation of behaviors and experiences which may be indicative of mental illness or psychological impairment. q. This is not the same as a “psychopath”. q. Analogy: Biologists study biology. Psychologists and Psychiatrists study psychology.
FIGURE 15. 4 The graph shows the breakdown of psychological disorders, comparing the percentage prevalence among adult males and adult females in the United States. Because the data is from 2007, the categories shown here are from the DSM-IV, which has been supplanted by the DSM-5. Most categories remain the same; however, alcohol abuse now falls under a broader Alcohol Use Disorder category.
HISTORICAL VIEWS OF MENTAL DISORDERS • Early views of mental disorders held to the somatogenic hypothesis. • Disorders are the result of a specific injury or infection. • Sigmund Freud, in contrast, argued for the psychogenic hypothesis. • Mental disorders are rooted in psychological processes.
MODERN THEORIES • Diathesis-stress model • Diathesis creates the predisposition or vulnerability. • Stress provides a trigger. • There also Protective Factors. • Biopsychosocial model • Multiple factors give rise to both diathesis and stress.
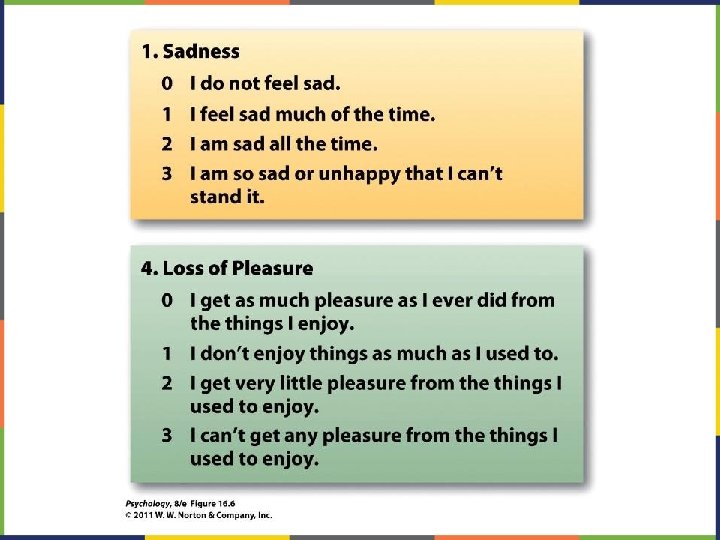
FIGURE 15. 5 Obsessive-compulsive disorder and major depressive disorder frequently occur in the same person.
FIGURE 15. 6 In The Extraction of the Stone of Madness, a 15 th century painting by Hieronymus Bosch, a practitioner is using a tool to extract an object (the supposed “stone of madness”) from the head of an afflicted person.
FIGURE 15. 8 A person’s risk of developing schizophrenia increases if a relative has schizophrenia. The closer the genetic relationship, the higher the risk.
DIFFERENT TYPES OF PSYCHOPATHOLOGY q. Psychopathology encompasses many different issues. q. These include, but are not limited to: depression, anxiety, schizophrenia, psychosis, bipolar depression, and personality disorders.
DEFINE, ASSESS, DIAGNOSE • A diagnosis is made with reference to the Diagnostic and Statistical Manual for Mental Disorders (DSM). The book now is the DSM 5. • The purpose of this book is to provide clinicians with a way to make a Clinical Case Formulation. • https: //youtu. be/G 9 sr. RI-XYr. M
CLINICAL CASE FORMULATION q. A Clinical Case Formulation is defined as a comprehensive assessment of someone. q. This includes knowing someone’s history, and a concise summary of their experiences with social, cultural, psychological factors.
CLINICAL CASE FORMULATION q. This then provides a solid overview to explain the reasons for why someone is experiencing the symptoms and the stressors they are currently going through. q. This then allows the clinician and client to find the better treatment plan options and overall treatment plan.
CLINICAL CASE FORMULATION q. Lets explore completing a clinical case formulation. You are about to view soap opera extremes of mental health issues in order to do that. These are not true. qhttps: //youtu. be/GYEkyxa. O 6 Bw qhttps: //youtu. be/fz 0 q 7 YKjp 48
QUIZ 1 q. How would you define the practice of psychopathology? q. How would you define a clinical case formulation? q. What are three things psychologists and therapist would look for when they are completing the clinical case formulation? q How would knowing these 3 things help with treatment planning?
ASSESSMENT • Assessment of any individual may include • semi-structured interview • The clinician evaluates symptoms and signs. • self-report measures • such as the Beck Depression Inventory • projective measures • such as the Thematic Apperception Test
ASSESSMENT • Assessment of any individual may include • semi-structured interview • The clinician evaluates symptoms and signs. • self-report measures • such as the Beck Depression Inventory • projective measures • such as the Thematic Apperception Test
DIAGNOSIS q. This is made after the assessment. q. The assessment provides you with a clinical case formulation. q. The clinical case formulation should always be flexible and ongoing. q. In order to be considered a diagnosis, the issues must cause a pervasive pattern or problems in many areas of a person’s life. q. Differential diagnoses, subtleties, unique.
ANXIETY DISORDERS q. Characterized by some level of fear and stress. q. One of the most common types of mental health issue. q. Separation Anxiety and Generalized Anxiety. q. PTSD, Social Anxiety, Phobias.
FIGURE 15. 9 Some of the physical manifestations of a panic attack are shown. People may also experience sweating, trembling, feelings of faintness, or a fear of losing control, among other symptoms.
FIGURE 15. 10 Worry is a defining feature of generalized anxiety disorder. (credit: Freddie Peña)
FIGURE 15. 11 (a) Repetitive hand washing and (b) checking (e. g. , that a door is locked) are common compulsions among those with obsessive-compulsive disorder. (credit a: modification of work by the USDA; credit b: modification of work by Bradley Gordon)
FIGURE 15. 12 Those who suffer from hoarding disorder have great difficulty in discarding possessions, usually resulting in an accumulation of items that clutter living or work areas. (credit: “puuikibeach”/Flickr)
ANXIETY DISORDERS • Generalized anxiety disorder. • continuous and pervasive feelings of anxiety • Obsessive-compulsive and related disorders. • obsessions (disturbing thoughts) and compulsions (repetitive behaviors). Also includes BDD, Trichotillomania, Skin Picking (Excoriation), and Hoarding. • The Trauma or Stress Related Disorders. • the result of identifiable and horrific events. • RAD, PTSD, Acute Stress, Adjustment Disorders, etc.
ANXIETY DISORDERS q. Panic attacks and panic disorder. q. Substance abuse or medication induced anxiety disorder. qhttps: //youtu. be/Ia. PN 9 KQo. Ybs qhttps: //youtu. be/htxw 16 Khvk. Y
GENES AND ANXIETY • A number of different genes are thought to contribute to the anxiety disorders. • Neuroimaging studies reveal that different anxiety disorders have different biological bases. • Conditioning accounts of anxiety disorders emphasize the role played by learning.
QUIZ 2 q. What is needed to consider someone’s symptoms a diagnosis? q. What is meant by differential diagnosis? q. What symptoms typically characterize an anxiety disorder? q. Please name two types of anxiety disorders.
DEPRESSIVE DISORDERS • Characterized by signs and symptoms that include a pervasive depressed mood and feelings of hopelessness. • Major Depression: issues with appetite, sleep, mood, motivation, lack of pleasure, feelings of worthlessness, and sometimes suicide or thoughts of death. • Persistent Depressive Disorder (Dysthymia): Chronic lower grade depression symptoms that last two years.
DEPRESSIVE DISORDERS • Mood disorders have important hereditary components. • A disruption of neurotransmission is also implicated, involving the norepinephrine, dopamine, and serotonin systems. • https: //youtu. be/d. Xeevtn 9_Os
DEPRESSION • Life crises often trigger depression. • However, crises by themselves do not cause the disorder. • Aaron Beck • negative cognitive schema • Explanatory style • Individuals who explain bad things that happen as the result of internal, global, and stable factors have an elevated risk of depression.
BIPOLAR AND RELATED DISORDERS q. Mania is the cardinal symptom of bipolar disorder. Without the mania, it would be considered Depressive Disorder. q. There are several types of Bipolar Disorder based upon the specific duration and pattern of manic and depressive episodes.
A MANIC EPISODE q. Inflated self-esteem or grandiosity (ranges from uncritical selfconfidence to a delusional sense of expertise). q. Decreased need for sleep. q. Intensified speech (possible characteristics: loud, rapid and difficult to interrupt, a focus on sounds, theatrics and self-amusement, non-stop talking regardless of other person’s participation/interest, angry tirades). .
A MANIC EPISODE q. Rapid jumping around of ideas or feels like thoughts are racing. q. Distractibility (attention easily pulled away by irrelevant/unimportant things). q. Increase in goal-directed activity (i. e. excessively plans and/or pursues a goal; either social, work/school or sexual) or psychomotor agitation (such as pacing, inability to sit still, pulling on skin or clothing).
A MANIC EPISODE q. Excessive involvement in pleasurable activities that have a high risk consequence. q. A Hypomanic Episode is very similar to a manic one, but less intense. It is only required to persist for 4 days and it should be observable by others that the person is noticeably different from his or her regular, non-depressed mood and that the change has an impact on his or her functioning.
BIPOLAR AND RELATED DISORDERS q. A Mixed Episode would fulfill the symptom requirements for both a Major Depressive Episode and a Manic Episode nearly every day but the mixed symptoms only need to last for a 1 -week period. q. The main difference between BP I and BP II is full mania (7 days) v. hypomania (4 days). Once a person experiences a full manic episode, they will receive a BP I diagnosis.
BIPOLAR AND RELATED DISORDERS qhttps: //youtu. be/D 933 -Im. Das. I
QUIZ 3 q. What factors characterize a depressive disorder? q. What are the differences between a depressive disorder and a bipolar disorder? q. Are there genetic components for people who eventually experience one of these types of mood disorders?
SCHIZOPHRENIA SPECTRUM AND OTHER PSYCHOTIC DISORDERS q. This illness is now considered a spectrum disorder. It's a group of related mental disorders that share some symptoms. They affect your sense of what's real. They change how you think, feel, and act. q. Delusional Disorder, Psychotic Disorders, Schizophreniform (similar to schizophrenia, less severe), and Schizoaffective (with mood episode).
SCHIZOPHRENIA SPECTRUM AND OTHER PSYCHOTIC DISORDERS • Someone with schizophrenia is likely to suffer from these symptoms: q 1. Delusions. 2. Hallucinations. 3. Disorganized speech (e. g. , frequent derailment or incoherence). 4. Grossly disorganized or catatonic behavior. 5. Negative symptoms (i. e. , diminished emotional expression or avolition)
SCHIZOPHRENIA q. At least two of the five symptoms must be present for at least one month. One of the two symptoms must be delusions, hallucinations, or disorganized speech. Negative symptoms, which impair function the most, are now official.
SCHIZOPHRENIA • Possible factors contributing to schizophrenia: • genetic predisposition • period of diminished oxygen supply to the newborn • a variety of prenatal viral infections • https: //youtu. be/y. L 9 UJVtg. PZY
SCHIZOPHRENIA • The evidence suggests that schizophrenia is a neurodevelopmental disorder. • Its precursors may be detected in early childhood. • Stress also contributes to schizophrenia.
QUIZ q. What are the five factors or symptoms associated with schizophrenia? q. Name two types of schizophrenia spectrum disorders. q. Are there genetic components in these disorders?
FIGURE 15. 13 Different regions of the brain may be associated with different psychological disorders.
FIGURE 15. 14 PTSD was first recognized in soldiers who had engaged in combat. Research has shown that strong social support decreases the risk of PTSD. This person stands at the Vietnam Traveling Memorial Wall. (credit: Kevin Stanchfield)
FIGURE 15. 15 Mood disorders are characterized by massive disruptions in mood. Symptoms can range from the extreme sadness and hopelessness of depression to the extreme elation and irritability of mania. (credit: Kiran Foster)
FIGURE 15. 16 Many medications designed to treat mood disorders work by altering neurotransmitter activity in the neural synapse.
FIGURE 15. 17 Depressed individuals react to negative emotional stimuli, such as sad faces, with greater amygdala activation than do non-depressed individuals. (credit: Ian Munroe)
FIGURE 15. 18 A study on gene-environment interaction in people experiencing chronic depression in adulthood suggests a much higher incidence in individuals with a short version of the gene in combination with childhood maltreatment (Brown & Harris, 2013).
FIGURE 15. 19 Longitudinal studies have helped to identify risk factors for predicting violent behavior.
PERSONALITY DISORDERS q. Personality is a complex set of characteristics that make us who we are, at least when it comes to our typical behaviors, ways of coping, and attitudes toward ourselves and others. Many regard our personalities as made up of dispositions that remain relatively consistent throughout our life situations and relationships. According to. Conscientiousness, Agreeableness, Neuroticism, Openness to Experience, and Extraversion.
PERSONALITY DISORDERS • Personality disorders involve traits or habits that characterize almost everything a person does. They must be shown to be pervasive in relationships. • These disorders are difficult to diagnose. • Diagnosis requires a very thorough history of how someone has behaved in their relationships with self and others.
PERSONALITY DISORDERS q. They fall within 10 distinct types: paranoid personality disorder, schizotypal personality disorder, antisocial personality disorder, borderline personality disorder, histrionic personality, narcissistic personality disorder, avoidant personality disorder, dependent personality disorder and obsessivecompulsive personality disorder.
PERSONALITY DISORDERS qhttp: //www. cbsnews. com/videos/mvp-brandon-marshall-on-bpd/ qhttps: //youtu. be/Pz. XB_1 xi--8 qhttps: //youtu. be/w. O 5 d 8 ig 48 XQ
QUIZ q. What is personality? q. What are the 10 personality disorders? q. How is personality disorder defined?
This Power. Point file is copyright 2014 -2015, Rice University. All Rights Reserved.