Poisoning in Children Norah Al Khathlan M D


















")
 –")


















- Slides: 46
Poisoning in Children Norah Al Khathlan M. D. Consultant Pediatrician Consultant Pediatric Intensivist 02/02/08
Poisoning in Children Goals: • Learn the pertinent aspects of the history and physical exam relative to acute poisoning with particular emphasis on clinical recognition of major toxic syndromes (toxidromes). • Understand the principles, methods, and controversies of decontamination and enhancement of elimination of toxins. • Learn the presenting signs, symptoms, laboratory findings, pathophysiology and treatment of common therapeutic drug poisonings, drugs of abuse, natural toxins and general household poisons.
Poisoning in Children Objectives: At the end of this lecture the student will be able to : 1. Define poisoning. 2. Identify specific Toxidromes. 3. Identify risk factors for pediatric toxidromes. 4. Differentiate between the different classes of toxidromes. 5. Differentiate the routes of poisoning. 6. Describe the general management of the toxidromes. 7. Outline the management of specific toxidromes: – – Iron Salicylates Paracetamole/ Acetaminophen Kerosene
Poisoning in Children • Definition of Poisoning: – Exposure to a chemical or other agent that adversely affects functioning of an organism. • Circumstances of Exposure can be intentional, accidental, environmental, medicinal or recreational. • Routes of exposure can be ingestion, injection, inhalation or cutaneous exposure. “All substances are poisons. . . the right dose separates poison from a remedy. ”
Poisoning in Children • Ingestion of a harmful substance is among the most • • common causes of injury to children less than six years of age Toxicology. . . is the science that studies the harmful effects of drugs, environmental contaminants, and naturally occurring substances found in food, water, air and soil. Poisoning maybe a medical emergency depending on the substance involved.
Poisoning in Children Constellation of signs & symptoms seen in poisoning characterized by the type of substance. Major four toxidromes are: – Anticholinergic – Sympathomimetic – Opiates/Sedatives- Hypnotics/ Alcohol – Cholinergic
Poisoning in Children Examples: • ASA • Acetaminophen • TCA • Narcotics & drugs of abuse • Benzodiazepines • Iron supplements • Alcohol
Agents Most Commonly Ingested by Children Less Than Six Years of Age, 1995 to 1998 Shannon M. N Engl J Med 2000; 342: 186 -191
Shannon M. N Engl J Med 2000; 342: 186 -191
Poisoning in Children Important history points • What toxic agent/medications were found near the patient? • What medications are in the home? • What approximate amount of the “toxic” agent was ingested? • • • – How much was available before the ingestion? – How much remained after the ingestion? When did the ingestion occur ? Were there any characteristic odors at the scene of the ingestion? Was the patient alert on discovery? – Has the patient remained alert since the ingestion? – How has the patient behaved since the ingestion? • Does the patient have a history of substance abuse?
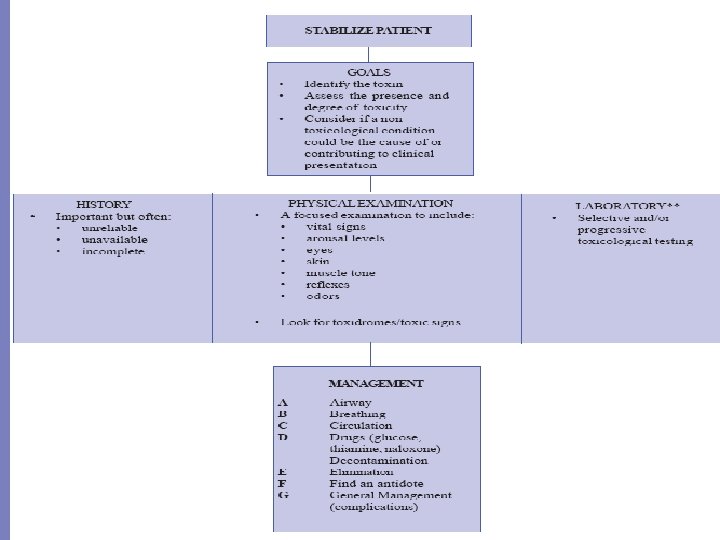
Poisoning in Children Management General measures: • Quick assessment & triage • Identify the culprit. • Limit absorption: – – – Vomiting Lavage Activated charcoal instillation Specific:
Poisoning in Children ABC’s of Toxicology: • Airway • Breathing • Circulation • Drugs: • Resuscitation medications if needed • Universal antidotes • Draw blood: • chemistry, coagulation, blood gases, drug levels • Decontaminate • Expose / Examine • Full vitals / Foley / Monitoring • Give specific antidotes / treatment
Poisoning in Children • Decontamination: 1. Ocular: – Flush eyes with saline 2. Dermal: – Remove contaminated clothing – Brush off – Irrigate skin 3. Gastro-intestinal: – Activated charcoal: – May Prevent /delay absorption of some drugs/toxins – Almost always indicated – Naso/oro-gastric Lavage – Bowel Irrigation: – – – Recent ingestions 4 -6 hrs Awake alert patient 500 cc NS Children / 2000 cc adults Orally / Nasogastric tube Contraindications…?
Agents Used for Gastrointestinal Decontamination in Children Shannon M. N Engl J Med 2000; 342: 186 -191
Circumstances under Which Administration of Ipecac Syrup Should Be Avoided Shannon M. N Engl J Med 2000; 342: 186 -191
Important points
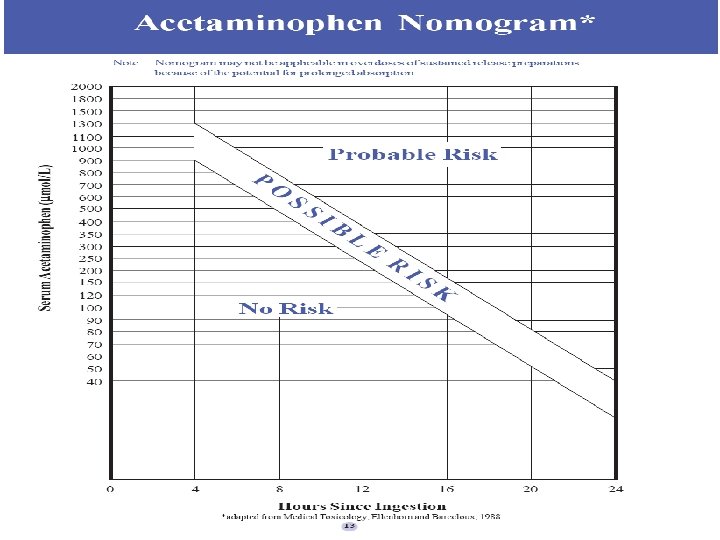
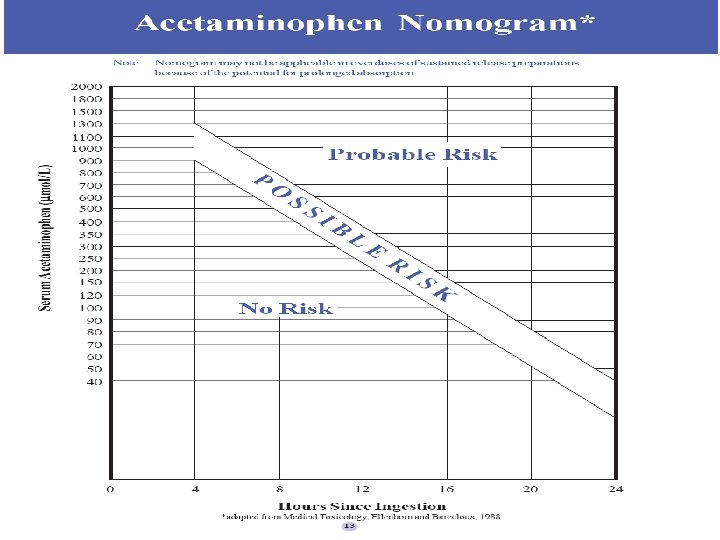
Specific toxidromes • Acetaminophen: – Stage I 0 -24 hrs • Early symptoms – – Mild Serum acetaminophen level 4 hrs post ingestion PLOT ON SPECIFIC NOMOGRAM. No need to repeat levels • If > 900 µmol/L ---> POSSIBLE RISK • Nausea, vomiting, malaise and diaphoresis. • Normal bilirubin Transaminases and PT
Acetaminophen poisoning • Stage II: – 24 -48 hrs after ingestion. • Better, less symptoms. • Elevated bilirubin, transaminases and PT
Acetaminophen poisoning • Stage III – 48 -96 hrs ( 2 - 4 days) after ingestion: • Hepatic dysfunction • (Rarely hepatic failure) • Peak elevations in: – Bilirubin – Transaminases may reach > 1000 IU/L – Prolonged PT
Acetaminophen poisoning • Stage VI – 168 - 192 hrs (7 -8 days) – Clinical improvement – LFTs returning to normal
Acetaminophen poisoning • Probable toxicity should be treated with: – N-acetylcysteine bolus 140 mg/kg – Then 70 mg/kg Q 4 hrs for 17 doses. – Assess hepatic function: • On presentation • Daily – Continue other support
Iron Poisoning • Five Stages but variable – Stage 1 • Gastro-intestinal stage: within several hrs of ingestion: – V/D. Hematochezia and abdominal pain – Severe: fluid loss, bleeding, shock(acidosis, tachycardia +/- hypotension) – Fever. Lethargy. Coma
Iron Poisoning • Stage 2 – Quiescent stage: 4 -48 hrs • Clinical improvement • Subtle hemodynamic changes: – Tachycardia – Decreased U. O. P.
Iron Poisoning • Stage 3: – Circulatory collapse : 48 -96 hrs • Metabolic acidosis, hypotension, low Cardiac output. • Coagulopathy • Multiorgan system failure
Iron Poisoning • Stage 4: – Hepatic failure: 96 hrs • Increased mortality • Rarely fulminant hepatic failure • Hepatic necrosis – Liver transplant can save lives
Iron Poisoning • STAGE 5: – Bowel obstruction 2 -6 wks – Due to scarring • Gastric outlet obstruction • Small intestinal obstruction – May not pass through stage 4
Iron Poisoning Management: 1. Gastric decontamination: • Forced emesis • Gastric lavage with 5% Na. HCO 3 • No activated char coal 2. Secure good IV 3. Get initial the 4 hrs levels and TBC 4. Chelate with Deferoxamine if levels> 300 mg/d. L
Iron Poisoning • Chelate with Deferoxamine: – Stable pts : levels< 500 mg/d. L 40 mg/kg IM/IV – Unstable: bleeding/ level > 500 • Give 20 cc/kg NS/RL • Deferoxamine at 15 mg/kg IV over 1 hr • Continuous drip at 15 mg/kg/hr • Continue till “vin rose” urine color disappears.
Iron Poisoning • Observe for: – – – Systemic BP ECG CVP – – Bleeding Glucose intolerance Hyperammonemia Encepalopathy • Signs of hepatic failure:
SALICYLATES • Oral ingestion commonest • Transdermal less • Peak levels at 12 hrs – Early : hyperpnea respiratory alkalosis – Then metabolic acidosis – Severe cases: Cerebral edema and increased ICP
SALICYLATES • MANAGEMENT – Treat electrolyte imbalance – IV hydration – Forced alkaline diuresis – Hemodialysis – Diuretics
Hydrocarbons • Kerosene ingestion: – – – Risk of aspiration GIT & Respiratory effects. Burning sensation, nausea, belching and diarrhea Cough, chocking, gagging and grunting. CXR 2 -8 hrs later: Pulmonary infiltrates or perihilar densities. – pneumatoceles, pleural effusion or pneumothorax and bacterial superinfection – Resolution 2 -7 days.
Hydrocarbons • Treatment: – Do not induce vomiting – Do not attempt gastric lavage – Risk of aspiration outweighs any benefit from removal of substance – CXR around 2 -4 hrs “not before 2 hrs” – Observe in ER for 6 -8 hrs if no symptoms discharge.
Poisoning in Children “Prevention is the vaccine for the disease of injury. ” • Host • AGENT • Environment A causal relationship!
Poisoning in Children “Prevention is the vaccine for the disease of injury. ” • Host • AGENT • Environment A causal relationship!
Poisoning in Children Prevention • The reduction in the incidence of childhood poisonings in the past • half-century has been dramatic. This reduction is largely the result of the combination of highly effective and passive methods of intervention. – Passive interventions eg: introduction of child-resistant containers for drugs and other dangerous household products. Child-resistant containers have been particularly effective in reducing the incidence of death from the ingestion of prescription drugs by children. – Active interventions, which require a change in behavior by parents and caretakers, include the safe storage of household products.
Thank you Norah Khathlan M. D.