Organophosphates POISONING Organophosphates Mechanism of Toxicity Clinical Features



 In children Seizures are more common (22%-25%). Lethargy and coma")
 Decontamination: a. Avoid further exposure b. Protection: gowns and")
 Stabilization: a. ABC’s: airway protection most commonly needed b. Orogastric lavage or")





 dizziness, confusion Paresthesia")

















- Slides: 51
Organophosphates POISONING
Organophosphates Mechanism of Toxicity •
Clinical Features (Acute Toxicity) In children Seizures are more common (22%-25%). Lethargy and coma (54%-96%). ØFlaccid muscle weakness, miosis, excessive salivation are common presenting signs.
TREATMENT 1. Initial management: (1) Decontamination: a. Avoid further exposure b. Protection: gowns and gloves c. Irrigation: ocular and dermal exposure d. Remove and discard clothing Skin should be washed repeatedly with water and soap. Cutaneous absorption can also occur as a result of contact with vomitus and diarrhea if the initial exposure was through ingestion
TREATMENT (2) Stabilization: a. ABC’s: airway protection most commonly needed b. Orogastric lavage or NG tube Activated charcoal (May need >1 dose!!) c. IV access for antidotes and fluids d. ECG and monitoring CXR and ABG (? aspiration) If VT, usually Torsades de Pointes Mg and maybe pacing
TREATMENT Benzodiazepines: Its effect appears to be more than the simple termination of seizures. Standard dosing should be used in all intubated or seizing patients
Carbamate poisoning
Organochlorine poisoning
Classification of Organochlorine Dichlorodiphenylethanes DDTMethoxychlor Hexachlorocyclohexane Lindane Cyclodienes Aldrin. Chlordane Dieldrin Endrin. Endosulphan. Hepatochlor Chlordecone (kepone) Winai Wananukul, Ramathibodi Poison Center Mirex
Acute Organochlorine Poisoning Prodomal symptoms: tremor, ataxia, quick involuntary jerk (myoclonus) dizziness, confusion Paresthesia of month, nausea, vomiting Winai Wananukul, Ramathibodi Poison Center
Acute Organochlorine Poisoning The typical presentation: Status epilepticus Followed by: Respiratory failure Cardiac arrhythmias Rhabdomyolysis & acute renal failure Winai Wananukul, Ramathibodi Poison Center
Treatment Control seizure as the same way as “Status ”epilepticus Phenobarbital Benzodiazepines Phenytoin Prevent ( )آﺘﺮﻭپیﻦ کﻨﺘﺮﺍ ﺍﻧﺪیکﻪ ﺍﺳﺖ complications Winai Wananukul, Ramathibodi Poison Center
Pyrethroid Poisoning
Classification of Pyrethrins & Pyrethroids Pyrethrins Cinerin IIJustmolin IJusmolin II Pyrethrin IIPyrethrum extract Type I Pyrethroids Allethrin Bioallethrin. Cismethrin. Kadethrin Permethrin. Phenothrin. Resmethrin. Tetramethrin Type II Pyrethroids Cyhalothrin. Cypermethrin. Cyphenothrin. Deltamethrin Fenpropenthrin Fenvalerate. Fluvalinate Winai Wananukul, Ramathibodi Poison Center
Pyrethroids Exposure Direct Toxic • Hypersensitivity • Allergic rhinitis Bronchial asthma Anaphylactic shock Local Irritation • Contact dermatitis Winai Wananukul, Ramathibodi Poison Center Corneal abrasion
Pyrethroid Poisoning: Human Usually mild Common: nausea and vomiting after ingestion of pyrethroids. Sever Cases: drowsiness, seizure and coma ( In patient exposed to large amount of pyrethroids, especially the product used in agriculture in higher concentration) Death from pyrethroid poisoning is rare. Winai Wananukul, Ramathibodi Poison Center
Management : Hypersensitivity Adrenaline Corticosteroids Bronchodilators Antihistamine : Direct Toxic Supportive treatment Winai Wananukul, Ramathibodi Poison Center
Herbicide LD 50 • Paraquat 150 • 2, 4 -D 375 • Alachlor 930 • Metribuzin 1, 100 • Dicamba 1, 707 • Atrazine 1, 780 • S-Metolachlor 2, 672 • Linuron 4, 000 • Clopyralid >5, 000 • Glyphosate >5, 000 • Imazapyr >5, 000 • Simazine >5, 000 mg/kg
COLOUR CHART FOR PRE-SCREEN 0 3 10 30 100 µg/m. L The limit of detection for paraquat in plasma and urine is about 2 -3 µg/m. L
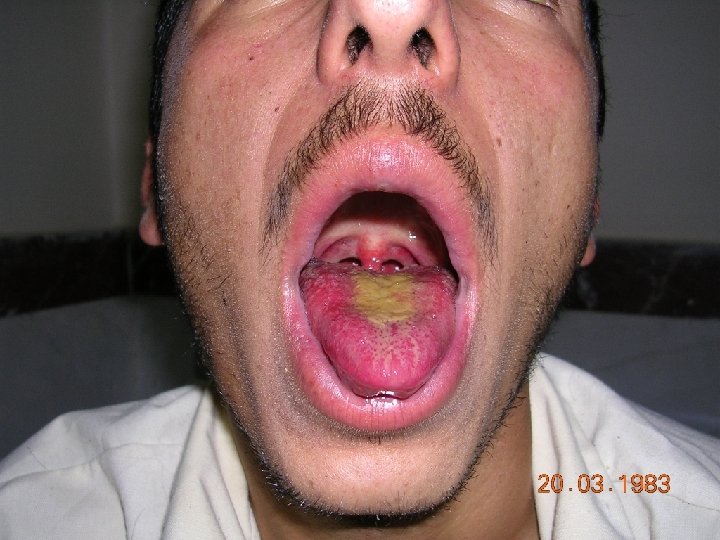
Glyphosate Abdominal pain with nausea, vomiting, and/or diarrhea are the most common manifestations of acute poisoning. inflammation, ulceration, or infarction dehydration. Gastrointestinal burns and necrosis Hemorrhage Severe poisoning manifests as multiorgan failure, including hypotension, cardiac dysrhythmias, kidney and liver dysfunction, hyperkalemia, pancreatitis, pulmonary edema or pneumonitis, altered level of consciousness including encephalopathy, and metabolic acidosis. These effects may be transient or severe, progressing over 12 to 72 hours to resistant shock, respiratory failure, and death. The mechanism of hypotension may relate to both hypovolemia (fluids shifts and increased losses) and/or direct cardiotoxicity. case fatality of 3. 2%----- from 2% to 30%.
Management observed for a minimum of 6 hours. Resuscitation and Supportive Care. All patients should receive prompt resuscitation, close observation, and routine supportive care; other treatments are largely empiric. Gastrointestinal Decontamination. Extracorporeal Removal. Patients who received hemodialysis have survived severe poisoning;
2, 4 -D AND MCPA Vomiting, myotonia , miosis. Gastrointestinal toxicity including nausea, vomiting, abdominal or throat pain, and diarrhea are common. neuromuscular findings (myalgia, rhabdomyolysis, weakness, myopathy, myotonia, and fasciculations), central nervous system effects (agitation, sedation, confusion, miosis), tachycardia, hypotension, kidney toxicity, and hypocalcemia. - death in one-third of the cases or 4. 4% Tachypnea with respiratory alkalosis---More severe poisoning may be characterized by metabolic acidosis, hyperventilation, hyperthermia, elevated creatine kinase, generalized muscle rigidity, progressive hypotension, pulseless electrical activity, or asystole.
Management continuous monitoring for 24 to 48 hours preferably in an intensive care unit. Resuscitation and Supportive Care. Gastrointestinal Decontamination Extracorporeal Removal- Hemodialysis should be considered in patients with severe poisoning if facilities are available urinary alkalinization increases the elimination of phenoxy herbicides. plasma and urinary (urine p. H > 7. 5) alkalinization