LEAD POISONING BENZENE POISONING Bodnar R Ya PLAN

LEAD POISONING BENZENE POISONING Bodnar R. Ya.

PLAN of lecture Lead poisoning Lead properties. Industrial uses. Pathogenesis of lead poisoning. Clinical picture. Diagnosis. Preventive measures. Management of lead poisoning. Benzene poisoning Benzene properties. Industrial uses. Pathogenesis of benzene poisoning. Clinical picture. Diagnosis. Management of benzene poisoning. Examination of working capacity.

LEAD POISONING

LEAD PROPERTIES low boiling point easily oxidised mixes with other metals easily to form alloys anticorrosive

LEAD COMPOUNDS lead arsenate lead oxide lead carbonate lead sulphide

INDUSTRIAL USES manufacture of storage batteries glass manufacture ship building printing and potteries rubber industry and several others

Lead smelter—the starting point of dissemination of a toxic metal

Rubber workers in mill room

Foundry workers may be exposed to a complex mixture of carcinogenic agents in fumes
 lead is gasoline. Thousands")
LEAD NON-OCCUPATIONAL SOURCES : The greatest source of environmental (non-occupational) lead is gasoline. Thousands of tons of lead every year is exhausted from automobiles. Lead is one of the few trace metals that is abundantly present in the environment. Lead exposure may also occur through drinking water from lead pipes; chewing lead paint on window sills or toys in case of children.

LEAD POISONING MODE OF ABSORPTION INHALATION INGESTION SKIN
 INHALATION: Most cases of industrial lead poisoning is due to inhalation")
LEAD POISONING (1) INHALATION: Most cases of industrial lead poisoning is due to inhalation of fumes and dust of lead or its compounds. (2) INGESTION: Poisoning by ingestion is of less common occurrence. Small quantities of lead trapped in the upper respiratory tract may be ingested. Lead may also be ingested in food or drink through contaminated hands. (3) SKIN: Absorption through skin occurs only in respect of the organic compounds of lead, especially tetraethyl lead Inorganic compounds are not absorbed through the skin.

LEAD DISTRIBUTION IN THE BODY: 90% of the ingested LEAD is excreted in the faeces. LEAD absorbed from the gut enters the circulation, and 95% enters the ERYTHROCYTES. It is then transported to the liver and kidneys and finally transported to the bones where it is laid down with other minerals. LEAD probably exerts its toxic action by combining with essential SH-groups of certain enzymes, for example some of those involved in prophyrin synthesis and carbohydrate metabolism.

LEAD POISONING CLINICAL PICTURE AFFECTION OF BLOOD SYSTEM AFFECTION OF NERVOUS SYSTEM AFFECTION OF GASTROINTESTINAL TRACT, LIVER

LEAD POISONING Stages of LEAD POISONING MILD MODERATE SEVERE

CLINICAL PICTURE AFFECTION OF BLOOD SYSTEM Syndrome of ANAEMIA (general weakness, fatigue, dizziness, paleness of skin) - is the early syndrome of chronic lead intoxication. ANAEMIA is hypochromic and associated with reticulocytosis and erythrocytosis (red blood cells with basophilic granularity).

red blood cells with basophilic granularity

AFFECTION OF BLOOD SYSTEM EARLY SIGN OF LEAD INTOXICATION – Affection of porphyrine metabolism which is manifested by rise of excretion with urine of Aminolevulinic acid and coproporphyrines with urine.

LEAD POISONING CLINICAL PICTURE AFFECTION OF BLOOD SYSTEM AFFECTION OF NERVOUS SYSTEM AFFECTION OF GASTROINTESTINAL TRACT, LIVER

CLINICAL PICTURE AFFECTION OF NERVOUS SYSTEM ASTHENIC SYNDROME NEUROPATHY ENCEPHALOPATHY

AFFECTION OF NERVOUS SYSTEM ASTHENIC SYNDROME Weakness Fatigue Disturbance of sleep Irritability Headache

AFFECTION OF NERVOUS SYSTEM NEUROPATHY Pain in extremities Paresis Paralysis

Pathways Leading to Pain in Peripheral Neuropathy

AFFECTION OF NERVOUS SYSTEM ENCEPHALOPATHY Headache, especially in the back of head, Dizziness Decline of memory Epileptiform attacks Mental confusion Delirium, etc

LEAD POISONING CLINICAL PICTURE AFFECTION OF BLOOD SYSTEM AFFECTION OF NERVOUS SYSTEM AFFECTION OF GASTROINTESTINAL TRACT, LIVER

AFFECTION OF GASTROINTESTINAL SYSTEM Dyspeptic syndrome (bitter taste in oral cavity, bad appetite, nausea, heartburn, eructation, sometimes vomiting) Pain syndrome (pain in epigastrium) Dyskinetic syndrome (constipation, diarrhea) Lead colic
Severe Abdominal pain 2) ↑ AP (>200/100) 3)")
AFFECTION OF GASTROINTESTINAL SYSTEM LEAD COLIC 1)Severe Abdominal pain 2) ↑ AP (>200/100) 3) Untreatable constipation

AFFECTION OF LIVER TOXIC HEPATITIS Liver is firm, painful, enlarged

DIAGNOSIS HISTORY OF LEAD EXPOSURE CLINICAL FEATURES -loss of appetite, -intestinal colic, -abdominal cramps and constipation, -persistent headache, -weakness, -joint and muscular pains, -BLUE LINE ON GUMS, -dermatitis, -anaemia, etc.

DIAGNOSIS Positive patch tests to acrylates in a worker who glued lead flashing onto window units. She had developed an allergic contact dermatitis affecting the hands.

DIAGNOSIS LABORATORY TESTS Measurement of lead in blood and urine Measurement of Coproporphyrin in urine

TREATMENT PRINCIPLES: To stop contact with a lead To get it out of organism - “complecsons” are widely used for lead destroying - “complecsons” form steady compounds with a lead and are easily extreted by kidneys with urine. Vitamine therapy (Vit. B 1, B 6, B 12, Vit. C) Dezintoxication therapy Sedative therapy Massage Warm bath Gymnastics

TREATMENT Tetacin-calcium and Pentacin are used for treatment of moderate and severe course of lead poisoning The use of d-penicillamine has been reported to be effective in treatment of mild course of lead poisoning

TREATMENT Tetacin-calcium i/v dr. 20 ml 10 % in 200 ml 5 % glucose during 3 days (with interruption - 3 -4 days), 2 -4 courses. You should remember that complecsons excrete from an organism different microelements which are needed for the vital functions of organism (iron, copper, cobalt), that’s why we must prescribe preparations of iron and vitamin B 12, which contains cobalt. ! Tetacin-calcium may cause exacerbation of pathological process in patients with the severe disturbance of the nervous system.

TREATMENT More effective is using of Pentacin 5% or 10% 20 ml i/v dr. for 3 days. 2 -3 courses are conducted with intervals in 5 days. Contraindications to application of pentacini are diseases of kidneys, arterial hypertension with violation of renal function.
 during 2 -4 weeks.")
TREATMENT D-penicillamine 150 mg in caps. (450 -600 mg/ day) during 2 -4 weeks.

TREATMENT Contraindications for using of complecsones are: - severe diseases of liver - severe diseases of kidneys - hemophilia - hypocalcemia

TREATMENT of intestinal colic Atropin 0, 1% 1 ml twice/ day Novocain blocking Sol. Glucose 5% + Vit. C 5% i/v Warm bath Hot-water bag
 Substitution : That is, where possible lead compounds should be substituted")
PREVENTIVE MEASURES (1) Substitution : That is, where possible lead compounds should be substituted by less toxic materials. (2) Isolation : All processes which give rise to harmful concentration of lead dust or fumes should be enclosed and segregated. (3) Local exhaust ventilation: There should be adequate local exhaust ventilation system to remove fumes and dust promptly (4) Personal protection : Workers should be protected by approved respirators. (5) Good housekeeping : Good housekeeping is essential where lead dust is present. Floors, benches, machines should be kept clean by wet sweeping.
 Working atmosphere : Lead concentration in the working atmosphere should be")
PREVENTIVE MEASURES (6) Working atmosphere : Lead concentration in the working atmosphere should be kept below 2. 0 mg per 10 cu. metres of air, which is usually the permissible limit or threshold value. (7) Periodic examination of workers : All workers must be given periodical medical examination. Laboratory determination of urinary lead, blood lead, red cell count, haemoglobin estimation and coproporphyrin test of urine should be done periodically. Estimation of basophylic stippling may also be done.
 Personal hygiene : Handwashing before eating is an important measure of")
PREVENTIVE MEASURES (8) Personal hygiene : Handwashing before eating is an important measure of personal hygiene. There should be adequate washing facilities in industry. Prohibition on taking food in work places is essential. (9) Health education : Workers should be educated on the risks involved and personal protection measures.

BENZENE POISONING

INDUSTRIAL USES Amino- and nitrogroups of benzene are wide-spread in industry: for making of organic dyes pharmaceutical preparations artificial resins Insecticides blasting matters

Electron micrograph of benzene particles Individual particles are about 25 nm in diameter

BENZENE COMPOUNDS aniline benzidin nitrobenzene nitrotoluol

BENZENE POISONING MODE OF ABSORPTION INHALATION INGESTION SKIN

BENZENE POISONING Amino- and nitro compounds of benzene, getting to the organism, accumulate in a -CEREBRUM, -KIDNEYS, -HEART, -LIVER. Then their redistribution occurs and most of matter stay too long in a temporal depot SUBCUTANEOUS-FATTY CELLULOSE and LIVER, that causes relapses of intoxication, particular after hot procedures and use of alcohol.

PATHOGENESIS During acute intoxication central NERVOUS SYSTEM and PERIPHERAL BLOOD are mainly affected (formation of methaemoglobin and development of hemolysis of erythrocytes occur). During chronic intoxication – LIVER, URINARY TRACTS, VISION ORGAN AND NERVOUS SYSTEM are affected.

BENZENE POISONING Intoxication by compounds of methaemoglobin causes development of irreversible degenerative changes in erythrocytes with formation of the rounded dark-blue inclusions on periphery - Gaints corpuscles. In the severe case the amount of methaemoglobin is increased to 6070 %, Gaints corpuscles - to 8 %.

Erythrocytes with Gaints corpuscles
.")
CLINICAL PICTURE Cerebral manifestations Acute headache, severe fatigue, nausea, vomiting, disorders of equilibrium (balance). Patients are disposed to syncope, depression. Cramps occur, tendon reflexes disappear. The loss of consciousness and comma appear. Patients may die from the paralysis of respiratory centre, heart failure. In the first days after the comma patient complains on intensive headache, weakness, dizziness.

CLINICAL PICTURE One of the most characteristic signs of acute intoxication of amino- and nitrocompounds is discoloration of skin. During examination grey-dark blue colouring of mucus and skin, cyanosis are revealed, dyspnoea is absent. Blood is of chocolate-brown colour; its colour depends on the quantity of formed methaemoglobin and sulfhaemoglobin.

CLINICAL PICTURE Amino- and nitrocompounds of benzene cause the irritation of mucus of respiratory tract that is accompanied by the sneeze, cough. Burns of nose mucus, nose-bleeding may occur.

CLINICAL PICTURE Urinary tracts are affected. Dysuric changes occur. In some cases , , haemolitic kidney” and acute renal failure. Acute toxic hepatitis. In some cases acute or subacute atrophy of liver occur and it is accompanied by the severe haemorrhagic syndrome and hepatic comma.

Results of blood investigations ↑methaemoglobin level ↑ conjugated bilirubin Geynts bodies Anizocytosis, Poycilocytosis, Erythrocytes with a basophilic stippling Reticulocytosis Blood viscosity rises. ↓ESR decreases.

BENZENE POISONING Stages of acute intoxication by amino- and nitrocompounds of benzene MILD MODERATE SEVERE

BENZENE POISONING MILD STAGE Patients complain on the headache, dizziness, weakness, sleepiness. At the objective examination cyanosis of mucus and skin of fingers, auricles, and uncertain step, rise of tendinous reflexes, tachycardia are revealed. Pathological changes of internal organs are absent.

BENZENE POISONING MILD STAGE Results of blood investigations: content of methaemoglobin in blood does not exceed 15 -20 %, single Geynts bodies. In a few hours after intoxication all these complaints pass, methaemoglobin level decreases, a work capacity recovers. Duration of intoxication does not exceed 24 days.

BENZENE POISONING MODERATE STAGE neurological symptoms: acute headache, dizziness, nausea, vomiting, severe muscles weakness, clouded consciousness. The patient orientation is broken, there is uncertain step. In these stage syncope may occur. At the objective examination: more expressed cyanosis of skin and mucus, pulse is labile, rise of tendinous reflexes, insignificant dyspnoea, poor reaction on light, insignificant expansion of heart, quit heart sounds, tahycardia. Sometimes liver is enlarged. Neurological status: nervous trunks are painful.
, ↑")
BENZENE POISONING MODERATE STAGE Results of blood investigations: ↑methaemoglobin level (to 30 -40%), ↑ little Geynts bodies (to 15%). Blood viscosity rises. ↓ESR decreases. Sometimes moderate leucocytosis. ↓content of oxygen in an arterial blood. The clinical-laboratory symptoms of intoxication are observed during 5 -7 days, although reverse development of basic manifestations of illness begins in 1 -2 days.

BENZENE POISONING SEVERE STAGE Severe changes of the central nervous system: Consciousness is cloded, often absent, cramps, dilation of pupils, disappearance of reaction on light, absence of tendon reflexes. In a acute period prostration is determined, it changes by acute excitement, involuntary urination and act of defecation. At the objective examination: severe cyanosis of skin and mucus, caused by connsiderable met- and sulfhaemoglobinemia and vein congestion. Skin hemorrhages, ulcer of mucus are revealed. Heart is delateted, heart sounds are decreased, tachycardia, decreasing of arterial pressure. Liver is enlarged and painful.

BENZENE POISONING SEVERE STAGE Results of blood investigations: ↑conjugated bilirubin in blood A blood is thick, chocolate-brown coloured, contains 60 -70 % methaemoglobin, a lot of Geynts corpuscles, anizocytosis, reticulocytosis, a lot of normoblasts and megaloblasts, leucocytosis may appear, ESR slows down.

CHRONIC BENZENE POISONING develops as a result of the protracted influence of small doses of poison that have cumulative action. Hot bath action, alcohol, the carried infection may cause exacerbation of chronic intoxication.

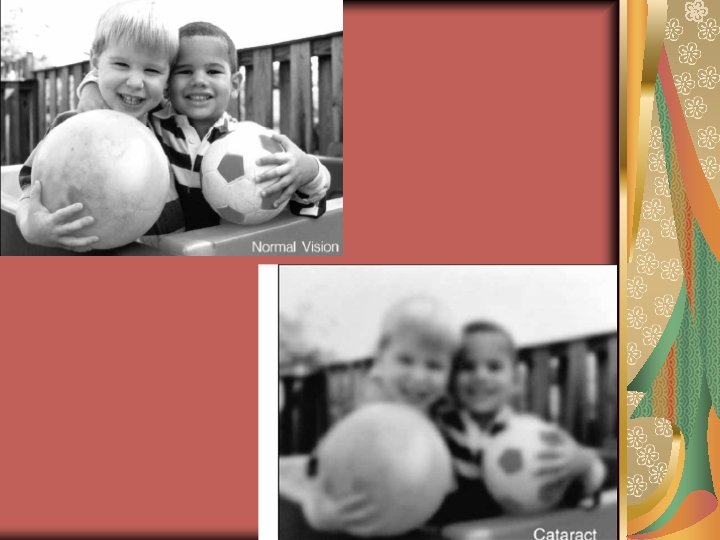
CHRONIC BENZENE POISONING CLINICAL PICTURE weakness, headache, dizziness, disturbance of sleep, rapid fatigue, dyspeptic symptoms, pain in right hypohondrium. Skin is pale, with cyanosis, colour of the eyes is icteric, pulse is labile, AP has a tendency to hypotonic. Heart sounds are decreased, chronic gastritis (frequently with decreased secretion), toxic hepatitis with moderate disturbance of liver function occur. The function of pancreas is affected. Disturbance of the urinary system occurs: chronic inflammation of mucus of urinary bladder, appearance of pappiloms of urinary bladder, malignant formations. Some benzene compounds cause occupational cataract.

BENZENE POISONING Occupational Cataract

ACUTE BENZENE POISONING DIAGNOSIS Diagnosis is made in case of contact of the patient with high concentrations of aromatic amino- and nitrocompounds (occupational anamnesis), characteristic clinical-laboratory symptoms: grey-dark-blue colour of skin and mucus, increased level of blood methaemoglobin and sulfhaemoglobin, appearance of Geynts corpuscles, erythrocytes with a basophilic stippling, reticulocytosis.

CHRONIC BENZENE POISONING DIAGNOSIS Diagnosis is based on a presence of complex of the exposed violations of blood, liver, nervous system, protracted contact with the indicated compounds.

BENZENE POISONING TREATMENT At acute intoxications patient should be taken out of the gassed atmosphere. At the getting of poison to skin it is necessary to wash soil area by water. Hot baths or showers are contraindicated. According to indications cardiac medicines are prescribed: camphora, coffein, cordiamin, corglycon. Desintoxication, vitamin and symptomatic therapy is recommended. At deppression of the central nervous system cytiton, lobelin are given. Oxygen therapy is the basic method of medical treatment.

BENZENE POISONING TREATMENT For reduction of blood viscosity - Glucose 40% 20 -30 ml i/v + Vit. C 5%. Glucose is a good demethaemoglobinisation mean. Use of vitamin B 12 is also recommended. In case of renal failure hemodialysis is conducted. During chronic intoxication medical treatment is conducted taking into account the clinical picture of disease.

EXAMINATION OF WORKING CAPACITY is made taking into account severity of the carried intoxication. At mild form after complete renewal of working capacity workers can go back to previous work. In the case of development of severe forms of intoxication after medical treatment, work out of contact with the toxic substances is recommended to the patient for the temporal time. At presence of the steady remaining pathological changes of different organs and systems, the work in contact with the toxic substances is stopped.

- Slides: 72