Pituitary Incidentalomas Fawn M Wolf MD 222018 Outline


")
:")





: – Common, screening")


 testing for all patients with a macroadenoma,")





:")
- Slides: 24
Pituitary Incidentalomas Fawn M. Wolf, MD 2/2/2018
Outline • • Prevalence Clinical presentation and evaluation Natural history Management
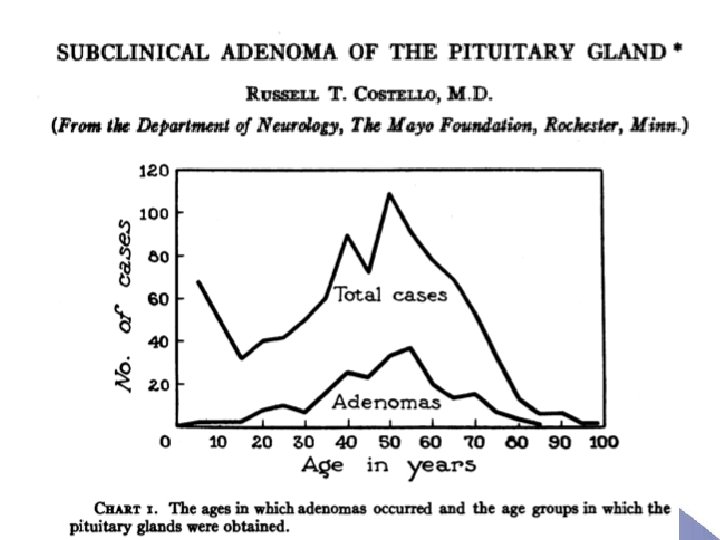
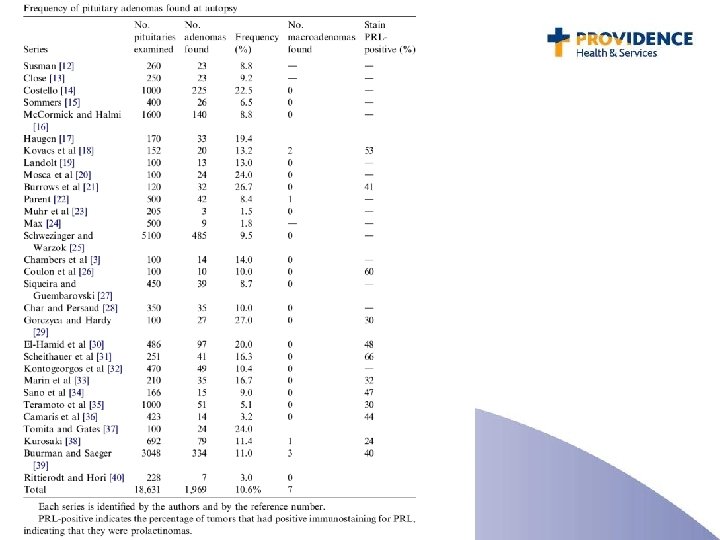
Over 18, 000 pituitaries examined at autopsy: -10. 6% contained adenomas (1. 5 -27%) -Frequency similar for men and women and across all age groups -Vast majority were microadenomas
Prevalence of Incidentalomas on Imaging • Incidentally discovered signal abnormalities < 10 mm (hypodensities): – CT: 4 -20% – MRI: 10 -38% • Incidental macroadenomas on CT/MRI are quite rare: 0. 1 -0. 2%
Differential Diagnosis of Incidental Pituitary Masses • • Adenoma: functional or nonfunctional Hyperplasia, infarction, hemorrhage Craniopharyngiomas, Rathke’s cleft cyst Meningioma Malignancy: metastases, primary pituitary Infiltrative: sarcoidosis, TB/fungal Inflammatory: hypophysitis (autoimmune, etc) Physiologic hypertrophy: pregnancy, puberty, primary hypothyroidism • Normal variant: large pituitary
Final Clinical Diagnoses of 282 Incidentalomas
Final Histopathological Diagnoses of Incidentalomas
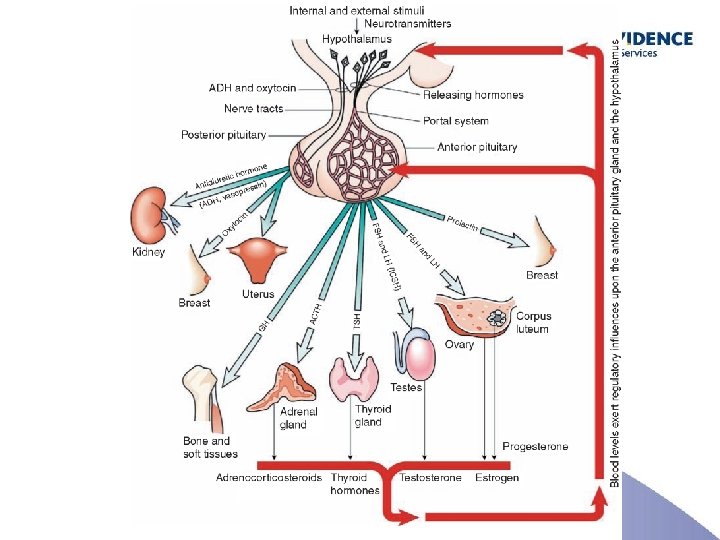
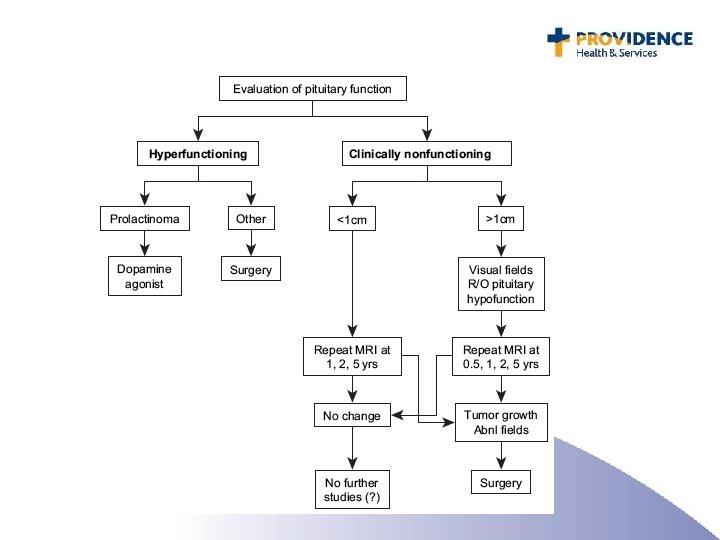
Pituitary Adenomas are Common Is it causing any: • Hormonal hyper secretion? • Hormonal hypo secretion? • Mass effects?
Endocrine Evaluation: Functional Adenomas • Prolactin. 10 -40% of adenomas are prolactinomas – ALWAYS test • Acromegaly (growth hormone): IGF-1. 2 -10% of adenomas are GH secreting. • Cushing’s disease (ACTH): cortisol. 1 -15% of adenomas are ACTH secreting. – Consider testing • FSH/LH • TSH – Generally don’t test
Endocrine Evaluation: Hypopituitarism • Macroadenomas and larger microadenomas (6 -9 mm): – Common, screening recommended • Smaller microadenomas (<6 mm): – Hypopituitarism rarely occurs – Screen only if clinically indicated
Evaluation for Hypopituitarism • FSH/LH: common, occurs in 30 -70% of patients – Pre-menopausal women: menstrual history • Normal: no labs needed • COCP: labs unhelpful • IUD: labs may be helpful, especially if FSH/LH and estradiol are low – Post-menopausal women: • No HRT: draw FSH, should be elevated • HRT: labs unhelpful – Men • FSH, LH, total +/- free testosterone
Evaluation for Hypopituitarism • ACTH: 20 -40% – Central adrenal insufficiency – 8 am cortisol or cosyntropin stimulation test • GH: 10 -50% – IGF-1: neither sensitive nor specific. Falsely low: obesity, insulin resistance. – Stimulation test: insulin, glucagon • TSH 20 -40% – Overtly low free T 4 (or significant drop from known baseline), with inappropriately normal or low TSH • PRL: – Inability to lactate; overtly low PRL typically only seen following apoplexy or with certain medications (aripiprazole)
Additional Work-up • Formal visual field (VF) testing for all patients with a macroadenoma, or a microadenoma abutting the optic nerves or chiasm, even if there are no apparent visual symptoms • Pituitary dedicated MRI (fine cuts though the sella w/w/o gadolinium), if initial study was a CT or brain MRI
Natural History of Incidental Nonfunctional Adenomas: Review of 8 Series
Natural History: 2016 Canadian referral based registry • 328 patients with incidentalomas included • 52% female, median age 55 years • 73% adenomas, of which 25% were functional and 36% had secondary hormonal deficiency (SHD) • 71% presented with macroadenomas
Natural History: Risk of growth and worsening hormonal status
Indications for Surgery • Visual field deficit, ophthalmoplegia or neurological compromise due to the lesion • Lesion abutting/compressing optic nerves or chiasm • Apoplexy with visual disturbance • Functional tumors, other than prolactinomas • Consideration of surgery: significant growth over time, hypopituitarism (with resolution in 15 -50% of patients), lesions close to the optic chiasm with plans for pregnancy
Take Home Points • Pituitary adenomas are very common: 10% prevalence on autopsy series • History and physical necessary to assess for visual compromise, hormonal hyper- or hyposecretion • Check prolactin in all pituitary incidentalomas, and consider screening for cushings and acromegaly • Macroadenomas: more likely to grow and cause visual compromise, also more likely to lead to hypopituitarism
References • 2016 Analysis and Natural History of Pituitary Incidentalomas. Eur J Encrinol 175(1): 1 -9 • 2012 Best Pract Res Clin Endocrinol Metab 26(1): 9 -19 • 2011 Pituitary Magnetic Resonance Imaging for Sellar and Parasellar Masses: Ten Year Experience in 2598 patients. J Clin Endocrinol Metab 96(6): 1633 • 2011 Natural History of Nonfunctioning Pituitary Adenomas and Incidentalomas: A Systematic Review and Metaanalysis. J Clin Endocrinol Metab 96(4): 905 • 2011 Pituitary Incidentaloma: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab 96(4): 894 • 2008 Nonfunctioning Pituitary Tumors and Pituitary Incidentalomas. Endocrinol Metab Clin N Am 37: 151. • 1994 Am J Neuroradiol. 15(4): 675 • 1994 Ann Intern Med. 120(10): 817 • 1997 Radiology 314: 287 • 1937 Am J Pathology Vol 12: 205