Pathophysiology of Pain Classification and Treatment Pain The

 defines pain as")














, • Hyperalgesia")


 for trigeminal neuralgia, • Gabapentin (Neurontin ) and transdermal")



 and duloxetine")
- Slides: 25
Pathophysiology of Pain, Classification and Treatment
Pain • The International Association for the Study of Pain (IASP) defines pain as “an unpleasant sensory and emotional experience which we primarily associate with tissue damage or describe in terms of such damage, or both. ” • Physical pathology does not need to be present for a patient to experience pain. • Composed of three hierarchical levels: • a sensory-discriminative component (e. g. , location, intensity, quality), • a motivational–affective component (e. g. , depression, anxiety), • a cognitive-evaluative component (e. g. , thoughts concerning the cause and significance of the pain)
Classification of Pain • According to pathology • Nociceptive • Neuropathic • Psychologic • According to duration • Acute • Subacute • Cronic (longer than 3 -6 months)
Nociceptive Pain Mechanisms • Clinically, pain can be labeled “nociceptive” if it is inferred that the pain is directly related to the degree of tissue injury. • Nociceptive pain is pain that is proportionate to the degree of actual tissue damage. • A more severe injury results in a pain that is perceived to be greater than that caused by a less severe injury. • Protective function • E. g. acute burns, bone fracture, and other somatic and visceral pains. • Nociception consists of four processes: transduction, transmission, modulation and perception.
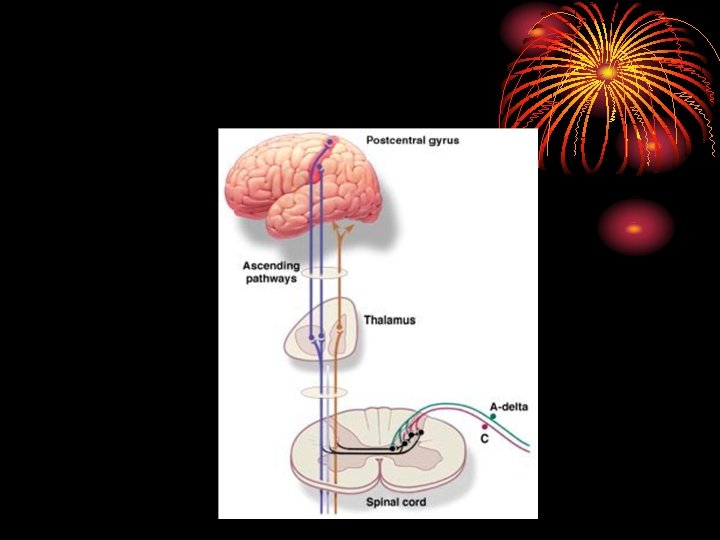
Nociceptive Pain Mechanisms • The detection of tissue damage by specialized transducers connected to A -delta and C-fibers • Anatomically, this process occurs predominantly peripherally and involves the nociceptor neurons, which terminate in the dorsal horn of the spinal cord.
• activation of specific receptors • depolarization of the peripheral nerve transduction
• Transmission: information proceeds proximally along the axon to the spinal cord and then on to higher centers. • Modulation: has been best characterized in the dorsal horn of the spinal cord.
• Pain-inhibitory and pain-facilitatory mechanisms • Inhibitory mechanism: • repetitive stimulation of primary A-beta mechanoreceptive neurons. • This is mediated through presynaptic inhibition in the substantia gelatinosa of the dorsal horn. • Facilitatory mechanism: • Long-term excessive impulse input from C-fiber nociceptive neurons (sensitization). • This long-term excessive input can be caused by chronic inflammation or other chronic noxious stimulation of C-fibers. • Descending facilitatory mechanisms also exist.
Pain-Inhibitory and Pain-Facilitatory Mechanisms Within the Dorsal Horn 0 A-BETA Neuronal circuitry within the dorsal horn. Primary afferent neuron axons synapse onto spinothalamic neurons and onto inhibitory and excitatory neurons. _ _ A-DELTA + STT + NEURON ++ TO BRAIN C
• Perception: Information that reaches the thalamus and other specialized brain structures may become recognized as pain. • Modulation: • endorphinergic system: analgesia is mediated by the binding of endogenous opioid compounds to different types of opioid receptors: mu, delta, and kappa. • monoamines (serotonin, norepinephrine and dopamine), histamine, acetylcholine
• Supraspinal control areas—including the reticular formation, midbrain, thalamus, hypothalamus, the limbic system of the amygdala and the cingulate cortex, basal ganglia, and cerebral cortex—modulate pain. Neurons originating from these cerebral areas synapse with the neuronal cells of the descending spinal pathways, which terminate in the dorsal horn of the spinal cord.
Neuropathic Pain Mechanisms • Neuropathic pain is the label applied to pain syndromes inferred to result from direct injury or dysfunction of the peripheral or central nervous system (CNS) • Peripheric mechanisms: • Membrane exitability • Peripheric sensitization • Cental mechanisms: • • Membrane exitability central sensitization Wind-up Loss of inhibition
Peripheral Sensitization Tissue damage and inflammation Norepinephrine, bradikinin, histamin Exitation threshold of nociceptors decreases (primary hiperalgesia) Mast degranulation (SP, histamin, seratonin ) Unexcitated nearby A delta and C fibers excitated (seconder hyperalgesia)
Central Sensitization • Ongoing of C nociceptive afferents • Longlasting DHN depolarization • İntracellular ca increases, NMDA recptors channells opened • Release of excitatory amino acids such as glutamate • Glutamate bind to (NMDA) res. • SP increases • Protein kinases C • NMDA res channels remains open
Loss of Inhibitory Interneuron Function • Under normal conditions, repetitive stimulation of A-beta mechanoreceptive afferents initially excites and then inhibits DHN (via interposed interneurons releasing GABA or enkephalin). • Denervation of input from A-beta afferent (deafferentation) or glutamate excitotoxicity.
0 A-BETA A-DELTA _ _ C Tonic activity in C nociceptors + STT + NEURON ++ ++ ++ TO BRAIN Enhanced postsynaptic effects by NMDA-receptor sensitization
• Allodynia (pain induced by nonnoxious stimuli, e. g. light touch), • Hyperalgesia (increased response to a noxious stimuli), • Hyperpathia (exaggerated responses to painful stimuli, with continuing sensation of pain after the stimulation has ceased).
• Peripheral neuropathic pain (e. g. , compressive or entrapment neuropathies, plexopathies, radiculopathies and polyneuropathies). • Central neuropatihc pain: depend on processes that predominantly reside in the spinal cord, brain or both (e. g. , pain due to spinal cord injury or poststroke pain).
Treatment
• Carbamazepine (Tegretol ) for trigeminal neuralgia, • Gabapentin (Neurontin ) and transdermal lidocaine (Lido. Derm ) for postherpetic neuralgia, • Duloxetine (Cymbalta) for diabetic neuropathy, • Pregabalin (Lyrica) for both diabetic neuropathy and postherpetic neuralgia • Serotonin-norepinephrine reuptake inhibitor (SNRI), antidepressants (eg, venlafaxine and duloxetine) and pregabalin are first-line medications for neuropathic pain.
Alpha 2 -Delta Ligands • Gabapentin was the first alpha 2 -delta ligand introduced to the market as an antiepileptic drug. • Adverse effects: somnolence, dizziness, gait and balance problems, gastrointestinal complaints and peripheral edema. • Start at a low dose (eg, 100 mg qhs to 300 mg qhs) and titrate upward. • Adjustments every 1 -7 days as tolerated by the patient. It may take several weeks to get to the target dose for an individual patient, and this may range from 1800 to 3600 mg per day.
• Pregabalin is another alpha 2 -delta ligand that is closely related to gabapentin. • The recommended starting dose is either 50 mg 3 times daily or 75 mg twice daily, with titration to 300 mg daily after several days. • Dosage of both gabapentin and pregabalin should be adjusted in patients with renal impairment.
Tricyclic Antidepressants • TCAs were among the earliest medications shown to have analgesic efficacy as "adjuvants" or "coanalgesics. " • Adverse effects can be considerable with the TCAs and include anticholinergic effects (eg, dry mouth, blurred vision, constipation, urinary retention, and cognitive impairment), sedation, and orthostatic hypotension. • Dosing should begin with 10 mg (older adults) or 25 mg at bedtime, and should be increased every 3 -7 days as tolerated. Generally, pain relief is achieved with 75 -100 mg per day.
SNRI Antidepressants • Venlafaxine (Effexor) and duloxetine