Pathophysiology of Pain PAIN is whatever a person



 ·")





 • Loc. :")
")






 5 Types HSAN 4 neurotroph tirozin-kináz receptor 1")



 Modulation of pain information by a gate")












 – Acetaminophen - NSAIDS: ASA, Advil, Motrin, Naprosyn,")





- Slides: 43
Pathophysiology of Pain
PAIN “…is whatever a person says it is and exists whenever the person says it does. ” (Mc. Caffery)
Pain 5 th Vital Sign · Should be recorded along with temperature, pulse, respiration, & blood pressure (American Pain Society)
Multidimensional Experience · Physical – Medical-Surgical conditions (special standards for acute post-operative pain) · Social – Support system & societal response · Psychological – Coping abilities, internal locus of control vs. external locus of control · Cultural – Emotionally expressive, introverted, stoic
Why it is necessary to study pain • Pain is the primary symptom that motivates people to seek medical treatment • Pain is subjective and therefore can only be measured indirectly
The Economic Cost of Pain in America · $100 billion/year related to chronic pain * includes healthcare expenses * compensation * litigation · Pain accounts for approximately: * 25% all sick days taken in US * 21% of emergency room visits (NIH, 2002)
Physiological Components of Pain
Transduction Noxious substance changes to an electrical stimulus by activating nociceptors (afferent nerve fibers that initiate the pain experience).
Pain Receptors and Periferal Afferent Pathways Stimulus impulse Information about possible tissue damage. · Specific theory (von Frey): – Distinctive end organs on the skin, each stimulus has specific end organ · Intensity theory: – Pattern or Summation Theory (Goldscheider): • Any sensory stimulus is sufficiently intense could produce pain. · Afferent fibers: – C fiber (0. 4 -1. 1 mm) – A-delta fiber (1 -5 mm)
Types of Nociceptors · C-nociceptors – Polymodal nociceptors (C-MH, mechano-heat sensors) • Loc. : skin 50 -70% • Stim. : >50 o. C, mechanical (biting, twinging), endogen substances (bradikinin, serotonin, acidic p. H), exogen substances (capsaicin etc. ) • Function: inflamatory pain and heat sensing. PGE 2 and PGI 2 potentiate the effect of bradikinin COX inhibitors • Signal transduction: VR-1 cation (Na+/Ca 2+ chanell) capsaicin and heat • Mediators: Substance P, CGRP and somatostatin • Substance P: neurogenic inflammation extravasation, leukocytosis, Ig secretion of B lymphocytes, TNF production of hystiocytes • CGRP: enhance microcirculation, potentiate neurogenic inflamation • Somatostatin: possible inhibits the inflammatory reactions
Types of Nociceptors · C-nociceptors – Heat receptors • Loc: skin 4%, (pig 30%) • Stim: heat, capsaicin and chemicals but mechanical stimuli not! – Chemoreceptors • Stim: electrical but heat and mechanical not. However they respond to repeated stimuli. (sleeping or silent receptors) – Others • High-Treshhold-Mechanociceptors (C-HTM): heat, capsaicin • C-Mechano-Cold (C-MC): Cold sensitive HTM receptors
Types of Nociceptors · A-delta Nociceptors – A-delta Mechano-Nociceptors • Loc: basal part of the epidermis and between of collagen fibers of joints • Stim: Hight-Treshhold-Mechanoreceptors sensing the pricking, cutting. Heat, capsaicin and irritants do not stimulate – A-delta Polynodal Nociceptors (AHH) • Loc: palm and hairless areas (Type I. ) Hairy areas (Type II. ) • Stim: mechanical • Function: Sensing of the first pain – Visceral Receptors
Transmission Passage of electrical impulse from the site of injury through the dorsal horn of spinal nerves & up the spinalthalmic tract to the brain.
Figure 10 -9: Sensory pathways cross the body’s midline
Substances That Stimulate Nociceptors: · Bradykinin: a powerful vasodilator that increases capillary permeability and constricts smooth muscle. Plays a role in chemistry of pain at site of injury. · Postaglandins: hormone-like substances that send additional pain stimuli to CNS · Substance P: believed to act as a stimulant at pain receptor sites and may influence inflammatory response
Neuromodulators: · Endorphins · Enkephalins · Dynorphin
Theories of pain • • Specificity model Patterning theory Gate control theory Multidimensional model
Hereditary Sensory and Autonomic Neuropathy (HSAN) 5 Types HSAN 4 neurotroph tirozin-kináz receptor 1 (NTRK 1) mutation Autosomal reseccive
Patterning Theory • Multiple neural pathways cause pain • Nociceptors plus other receptors • Cannot fully account for subjective nature pain
If you hurt yourself, you often rub the affected area to make it feel better. Why does this work?
Counter Irritant Theory · Gate Control Theory – Gate Cells – Tract Cells · Touch Input – Ab Fibers · Local Inhibition – GABA and Enkephalin
Gate Control Theory (Melzack & Wall 1960’s) Modulation of pain information by a gate mechanism From pain fibres Gating Mechanism Transmission cells Spinal cord From other peripheral fibres
Descending Pain Control · Cingulate Cortex · Periaqueductal Gray – Opiod Receptors – Projects to Raphe Nuclei · Raphe Nuclei – Project down to dorsal horn and Spinal 5 Nucleus – Serotonin (5 -HT) – Inhibits Ascending Systems • Substance P release by Primary Afferents · Locus Coeruleus – Norepinephrine · Hormonal Analgesia
Gate Control Theory • Accounts for high pain perception with Low damage (e. g. back ache) • Accounts for low pain perception with high damage (e. g. sport, bed of nails) • Does not fully account for reinforcement/ learning and environmental influences
Multidimensional model This model is consistent with Gate Control Theory and distinguishes four dimensions of pain: • Nociception - neural detection • Sensation - experience of pain (e. g. intensity) • Emotion - emotional response (e. g. anxiety) • Behaviour - e. g. withdrawal
Multidimensional model Physiological Learning ? Sensation Environment ? Emotional response Behavioural response e. g. tension e. g limping
Psychosocial Determinants of Pain • Emotional response • Cognition • Conditioning • Cultural/social context
Emotional response • Stress/Anxiety: Associated with pain • Motivation reduces pain, e. g sport. Possible opioid mechanism. • Depression: associated with increased pain.
Cognitive response • Appraisal e. g. pain is perceived as greater when it is life threatening • Higher self-efficacy = less pain • Expectations e. g. anxious dental patients expect more pain and therefore experience more pain
Conditioning • Reinforcement e. g. children with eczema who receive more attention in response to their pain behaviour are likely to increase their pain behaviour
Culture • e. g Bedouin women report less pain during child birth than in other cultures because it is not culturally acceptable to report pain
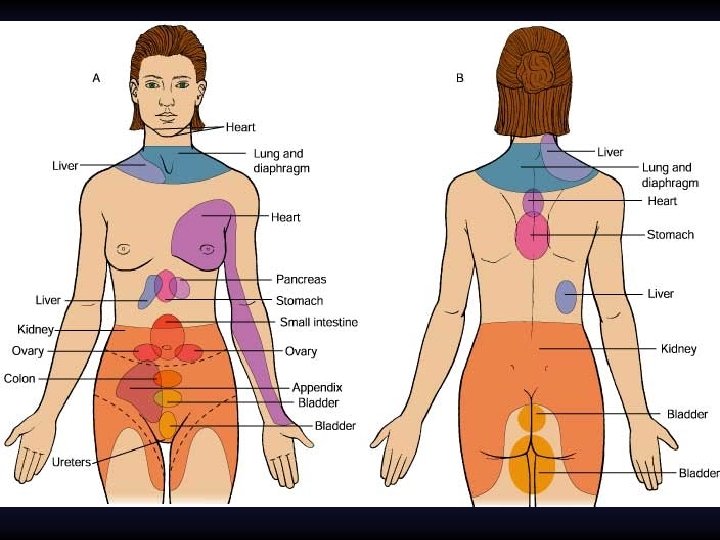
Types of Pain · Somatic – Smooth muscle walls, receptors in abdominal cavity, cranium, & thorax · Visceral – Arises from ligaments, tendons, bones · Referred – Pain experienced from a site distant from injury · Phantom – Sensations of burning, tingling felt in absent limb · Neuropathic – Pain signal from injury to higher centers of brain
Acute Pain vs. · Usually sudden, self· · · limiting < 6 months Precipitating event Resolves with treatment Restless, anxious, crying Chronic Pain · May be sudden or · · · gradual with periods of remission & exacerbation > 6 mo. May not be associated with injury Difficult to treatment Depressed, withdrawn
Classification of Analgesics · Non-opiod (non-narcotic) – Acetaminophen - NSAIDS: ASA, Advil, Motrin, Naprosyn, Feldene Toradol (Ketorolac) Cox – 2 Inhibitors (Vioxx & Celebrex) - Side Effects: Gastric erosion, GI bleeding, fluid retention, Platelet dysfunction, & renal insufficiencies
Classification of Analgesics Opiod Analgesics: Synthetic Narcotics Commonly Used: - Morphine Sulfate, Oxycontin - Dilaudid (hydromorphone) - Oxycodone (Percodan, Percocet, Oxycontin SR - Demerol (Meperidine) - Fentanyl - Codeine Plain - Tylenol 300 mg - # 2 (15 mg), # 3, (30 mg) # 4 (60 mg) - Vicodin (Hydrocodone 5/500, 7. 5/750, 10/660
Non-pharmacological Interventions · · · · · Heat & cold Progressive relaxation Massage Meditation, Guided Imagery Music Biofeedback Transcutaneous Electric Nerve Stimulation Therapeutic Touch Yoga
Invasive Pain Management · Epidural · Intrathecal · Nerve Blocks