Dysfunctional Uterine Bleeding Dr Mona ElTalatini ST 7

Dysfunctional Uterine Bleeding Dr. Mona El-Talatini ST 7, Queen Medical Centre, Nottingham
 Etiology")
Discussion Points • • • Definition Epidemiology Classification of abnormal uterine bleeding (AUB) Etiology Diagnosis Investigation Treatment Follow up Complication Summary

Definition of DUB • Excessive uterine bleeding affecting pre-menopausal women that is not due to pregnancy or any recognizable uterine or systemic diseases. • The underlying pathophysiology is believed to be due to ovarian hormonal dysfunction.

Epidemiology • 25% of Women-One episode. • 5% of women aged 30 -49 years in UK. • Only Quarter of women with excessive bleeding seek medical treatment. • DUB affects women at extremes of their reproductive age and women suffering from chronic anovulation(PCOS).
 Menstrual")
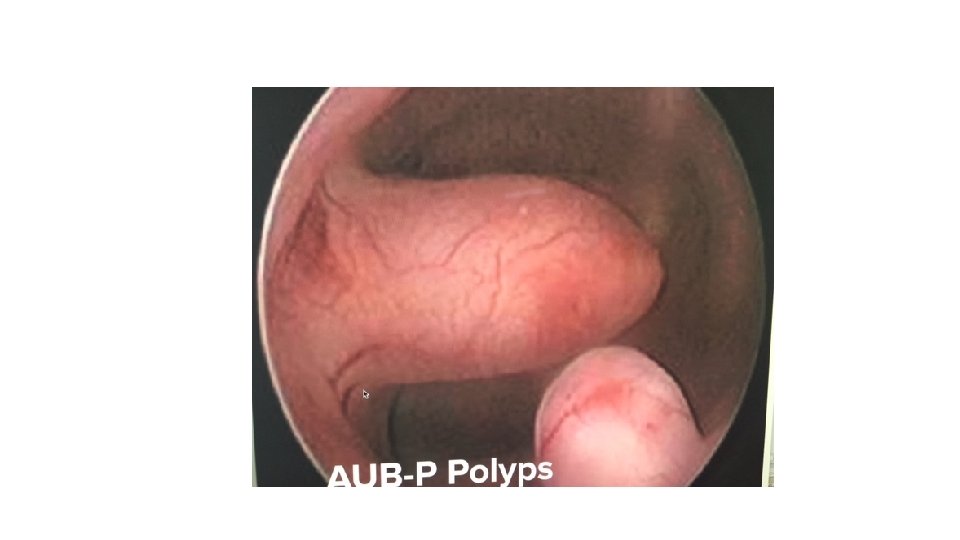
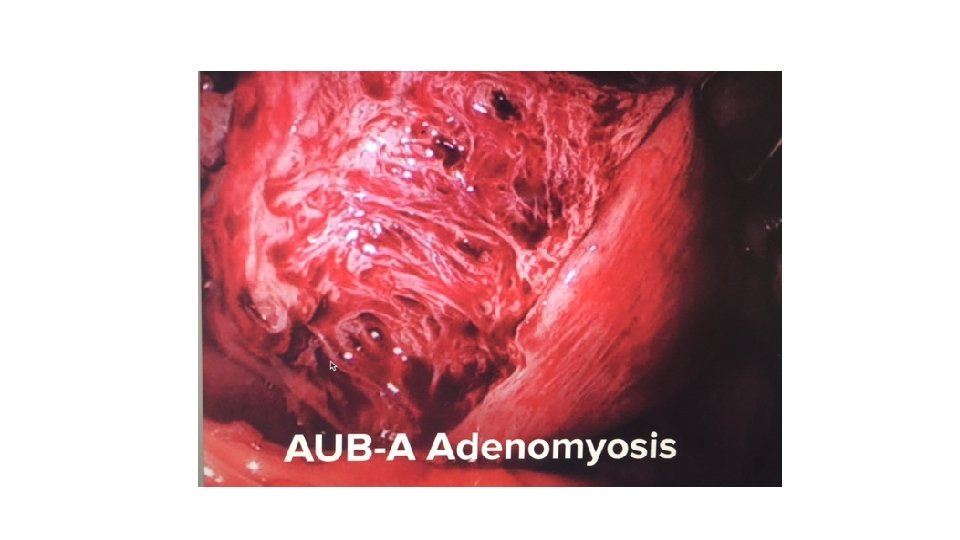
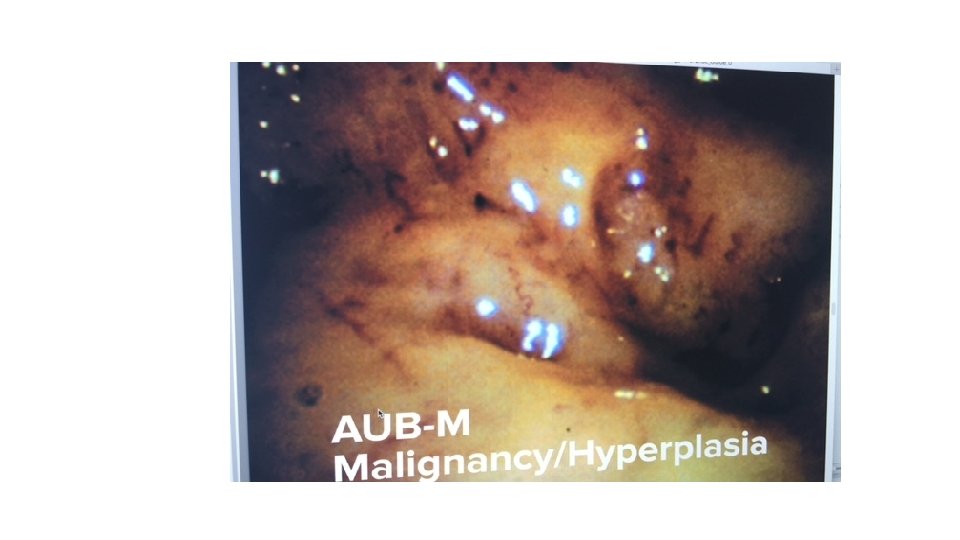
Classification of Abnormal uterine Bleeding v. International Federation of Gynecology and Obstetrics (FIGO) Menstrual Disorders Group(2011): • 1. structural causes for AUB: polyp; adenomyosis; leiomyoma; malignancy and hyperplasia. • 2. non-structural causes for AUB: coagulopathy; ovulatory dysfunction; endometrial; iatrogenic; and not yet classified. v. DUB is not included in classification. vgenerally fit ovulatory dysfunction and endometrial hemostatic disorders if coagulopathy has been excluded.

PALM-COEIN classification system for abnormal uterine bleeding in non gravida reproductive-age women, 2011

 v. Dysfunctional uterine bleeding (DUB) : • ovulatory or anovulatory HMB but")
DUB (AUB-O) v. Dysfunctional uterine bleeding (DUB) : • ovulatory or anovulatory HMB but mainly due lack pf ovulation. • This is diagnosed after the exclusion of pregnancy, medications, iatrogenic causes, genital tract pathology and systemic conditions.
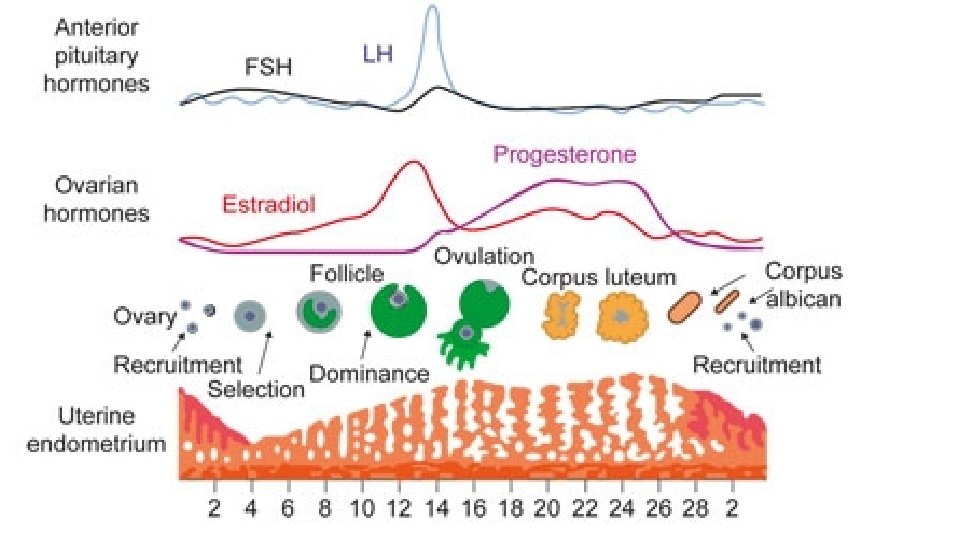

Etiology • Disorders that interfere with ovarian follicular development resulting in ovulatory dysfunction (either anovulation or defective ovulation with abnormal corpus luteum formation) are known to be associated with DUB. • These include polycystic ovary syndrome, hyperprolactinaemia, hypothalamic anovulation , and hypothyroidism.
, Duration,")
Clinical Assessment : History: • Age • Menstrual history: Cycle (22 d-35 d), Duration, Volume, frequency • IMB, PCB • Associating symptoms Pelvic pain, Anemia, impact on quality of life. Fertility wishes • CX smear • Contraception • Medical history: Endocrine disorders such as thyroid, hyperprolactinemia, PCOS problems • PH/ FH of inherited hemophilia , thrombocytopenia Gynae cancer, thromboembolism, Liver disease.

Physical examination ØBMI , PCOS signs Ø Signs of anemia. ØAbdominal and pelvic examination: Speculum: cervical cytology if appropriate genital tract infection screening: cervicitis/endometritis is suspected on history or examination. Bimanual examination of uterus : fibroids.

Investigations • 1. Pregnancy test • 2. FBC, • coagulation profile • 3. Hormonal investigations; PRL, Thyroid , Testosterone , FSH, LH • 4. Pelvic scan
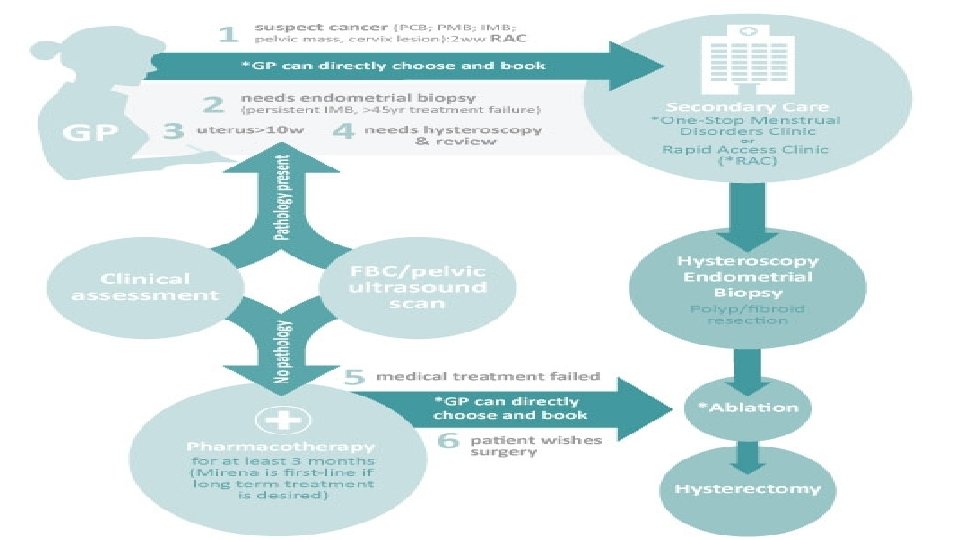

Red Flag features of AUB indicating 2 ry care referral Pathology suspected before treatment 1. Suspected Gynaecology cancer 2. Requires endometrial biopsy (to rule out endometrial hyperplasia or endometrial cancer). PCB, IMB, Pelvic mass or Cervical lesion o. Persistent IMB o>45 years with treatment failure o. Irregular bleeding while on HRT or tamoxifen Pathology suspected before after treatment 3. Enlarged uterus (clinically measures >10 weeks size or >10 cm uterine cavity length). 4. Moderate/severe anaemia on FBC. . Uterine/ovarian pathology identified on ultrasound scan. . Identification of coagulation/haemostatic disorder on clinical screening and testing Fibroids, adenomyosis Pathology suspected after treatment 5. Medical treatment has failed § At least 3 months of drug treatment (at least 6 months of Mirena) and failure is based on woman’s own assessment. 6. Patient wishes for surgery Fibroid e. g. von Willebrand disease § Endometrial ablation, hysterectomy

Primary options Progestogens Northiosterone: 5 mg TDS D 5 -D 26 OR medroxyprogesterone: 5 -10 mg orally once daily for 5 -10 days of each month, start on days 16 -21 of cycle OR progesterone micronised: 200 mg orally once daily for 12 days of each month *levonorgestrel intrauterine device: OR etonogestrel subdermal implant/injection Non-Steroidal anti-inflammatory drug (NSAID) CI: Peptic ulcer and bronchial asthma Antifibrinolytic agents [C Evidence] 2 ndry options COCpills useful when the use of oestrogens and progestogens are contraindicated. [B Evidence] mefenamic acid: 500 mg orally as a single dose initially, followed by 250 mg every 6 hours when required OR ibuprofen: 400 -800 mg orally every 6 -8 hours when required, maximum 2400 mg/day OR naproxen: 250 mg orally every 6 -8 hours when required, maximum 1250 mg/day tranexamic acid: 1 g orally three times daily for up to 4 days during menstruation

Follow up q. Monitoring • longstanding DUB, those associated with anovulation, to be monitored due to the increased risk of endometrial hyperplasia and endometrial cancer. • To identify failed medical treatment. • q. Patient instructions • Menstrual diary. This gives valuable information on the amount and extent of bleeding and is useful in monitoring response to treatment.

Complications • Endometrial hyperplasia/cancer • Anemia

Summery • AUB Classification • Clinical assessment: history, clinical examination, investigations • Management • Referral to the hospital • Follow up • Complications
. Heavy menstrual bleeding. 2007")
References • National Institute for health and Clinical Excellence (NICE). Heavy menstrual bleeding. 2007 updated August 2016. • Munro MG, Critchley HO, Broder MS, Fraser IS and the FIGO Working Group on Menstrual Disorders. FIGO classification system (PALM-COEIN) for causes of abnormal uterine bleeding in nongravid women of reproductive age. Int J Gynaecol Obstet 2011; 113: 3– 13 • Dysfunctional uterine bleeding. Best practice; BMJ 2015
- Slides: 24