Oesophagal Diseases Gastroesophageal Reflux Disease GERD ACG define

 ACG define – Symptoms or mucosal damage produced by the")






, alcohol, caffiene,")
 stricture")




")
 § Esophageal manometry (absent peristalsis,")







")









 there")

")


- Slides: 40
Oesophagal Diseases
Gastro-esophageal Reflux Disease (GERD) ACG define – Symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus which are Often chronic and relapsing.
• Pathophysiology
• Clinical Presentations of GERD • Heart burn is a classical symptom- Substernal burning or regurgitation, Postprandial, Aggravated by change in position, get releif by Antacid. • Potential Oral and Laryngopharyngeal Signs Associated with GERD - Edema and hyperemia of larynx, Vocal cord erythema, polyps, granulomas, ulcers • Hyperemia and lymphoid hyperplasia of posterior pharynx • Interarytenyoid changes
• Clinical Presentations of GERD • Hoarseness, Laryngitis, • Pharyngitis, Chronic cough, Globus sensation, Dysphonia, • Subglottic stenosis, Laryngeal cancer. • Pulmonary symptoms are Asthma, Aspiration pneumonia, Chronic bronchitis, Pulmonary fibrosis. • Chest pain, Dental erosion
Diagnostic Tests for GERD • Barium swallow • Endoscopy
• Ambulatory 24 hr p. H monitoring. • Esophageal manometry - Assess LES pressure, location and relaxation, Assist placement of 24 hr. p. H catheter Assess peristalsis - Prior to antireflux surgery
Treatment Goals for GERD 1. Eliminate symptoms 2. Heal esophagitis 3. Manage or prevent complications 4. Maintain remission
Ø Lifestyle modifications • Avoid large meals • Avoid acidic foods (citrus/tomato), alcohol, caffiene, chocolate, onions, garlic, peppermint • Decrease fat intake • Avoid lying down within 3 -4 hours after a meal • Elevate head of bed 4 -8 inches • Avoid meds that may potentiate GERD (CCB, alpha agonists, theophylline, nitrates, sedatives, NSAIDS) • Lose weight, Stop smoking. Ø Acid Suppression Therapy- PPI Ø Antireflux surgery
Complications of GERD Erosive/ulcerative esophagitis Esophageal (peptic) stricture
• Balloon Dilation of a Peptic Stricture
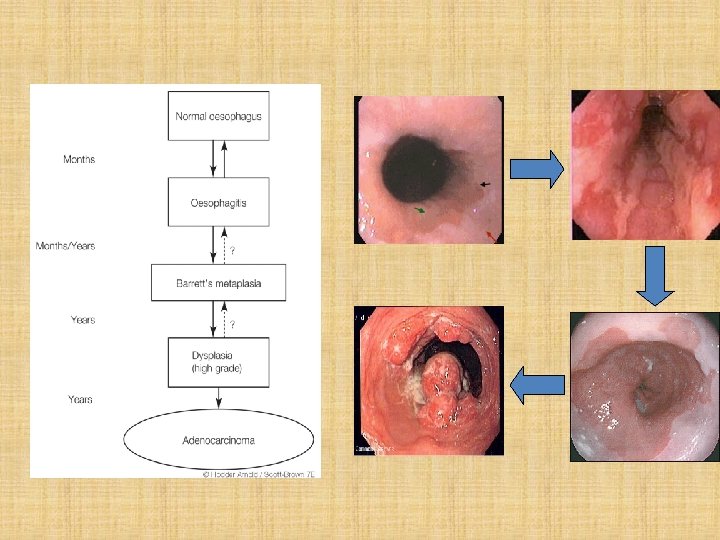
Barrett’s Esophagus • Defined as the presence of >3 cm of Columnar lined esophagus. • Incidence 0. 5 -2% • Associated with the development of adenocarcinoma
Motility Disorders • Achalasia • Diffuse esophageal spasm • Nutcracker esophagus • Scleroderma • Nonspecific esophageal dysmotility
Achalasia • Achalasia means “failure to relax. ” term coined in 1929 • Epidemiology 1 -2 per 200, 000 population usually presents between ages 25 to 60 male=female Pathophysiology • loss of ganglionic cells in the myenteric plexus (distal to proximal)----that affect relaxation of LES. • Basal LES pressure rises
• Clinical presentation solid dysphagia 90 -100% (75% also with dysphagia to liquids) post-prandial regurgitation 60 -90% chest pain 33 -50%, weight loss nocturnal cough and recurrent aspiration Diagnostic Work Up § Barium esophagram (dilated esophagus with taper at LES) Bird peak , § good screening test (95% accurate)
§ Endoscopy (rule out GE junction tumors, esp. age>60) § Esophageal manometry (absent peristalsis, LES relaxation, & resting LES >45 mm. Hg
Treatment of Achalasia • Nitrates and Calcium Channel Blockers- Reduces LES pressure. • Balloon Myotomy-Sequential dilation of LES with intraluminal ballons of 30, 35 & 40 mm under flurocopic control. • Surgical Myotomy by either an Open or Laproscopic approach. A laparoscopic Heller myotomy and partial fundoplication is the procedure of choice for esophageal achalasia.
Diffuse Esophageal Spasm • Unknown etiology. • Nonprogressive dysphagia with solids and liquids and nonexertional chest pain that responds to nitroglycerin. • corkscrew on barium. • The diagnosis by manometry periodic occurrence of simultaneous highamplitude contractions with intervening periods of normal peristalsis. • Treatment: -Nitrates, and CCBs , Botulinum toxin injection, surgery does not have an established role.
Nutcracker Esophagus • high pressure peristaltic contractions • avg pressure in 10 wet swallows is >180 mm Hg • 33% have long duration contractions (>6 sec) • may inter-convert with DES
Esophageal Webs • localized narrowing of the esophagus caused by intraluminal extension of the mucosa and part of the submucosa • Congenital or acquired (mc), usually secondary to conditions such as iron deficiency anemia/Plummer-Vinson syndrome and ulcerative colitis. • Tt: endoscopic dilatation
Pharyngoesophageal/Zenker’s Diverticula • From muscle incoordination that leads to herniation of the mucosa in prox esophagus. • Dysphagia mc symptom, halitosis, regurgitation, throat discomfort, palpable neck mass, recurrent aspiration pneumonia. • The best initial diagnostic tool is a barium swallow.
Carcinoma Esophagus
• Epidemiology: • Esophageal cancer is the 7 th leading cause of cancer deaths, accounts for 1% of all malignancy & 6% of all GI malignancy. • Most common in China, Iran, South Africa, India and the former Soviet Union. • The incidence rises steadily with age, reaching a peak in the 6 th to 7 th decade of life. • Male : Female = 3. 5 : 1 • Worldwide SCC responsible for most of the cases. • Adenocarcinoma now accounts for over 50% of esophageal CA, due to association with GERD , Barretts’s esophagus & obesity. • SCC usually occurs in the middle 3 rd of the esophagus (the ratio of upper : middle : lower is 15 : 50 : 35). • Adenocarcinoma is most common in the lower 3 rd of the esophagus, accounting for over 65% of cases.
Ø Risk Factors : Squamous Cell Carcinoma • Smoking and alcohol (80% - 90%) • Dietary factors – N-nitroso compounds (animal carcinogens) – Pickled vegetables and other food-products – Toxin-producing fungi – Betel nut chewing, Ingestion of very hot foods and beverages (tea) • Underlying esophageal disease (such as achalasia and caustic strictures) • Genetic abnormalities: p 53 mutation Ø Risk Factors: Adenocarcinoma • • Associated with Barretts’s esophagus, GERD & hiatal hernia. Obesity (3 to 4 fold risk) Smoking (2 to 3 fold risk) Increased esophageal acid exposure such as Zollinger-Ellison syndrome.
Clinical Features • Associated with the symptoms of dysphagia, wt. loss, pain, anorexia, and vomiting • Symptoms often start 3 to 4 months before diagnosis • Dysphagia - in more than 90% pt. Odynophagia - in 50% of pt. • Wt. loss – more than 5 % of total body wt. in 40 – 70% pt. associated with worst prognosis. Complications: • Cachexia, Malnutrition, dehydration, anaemia, . • Aspiration pneumonia. • Distant metastasis. • Invasion of near by structures: e. g. – Recurrent laryngeal nerve → Hoarseness of voice – Trachea → Stridor & TOF→ cough, choking & cyanosis – Perforation into the pleural cavity → Empyema
Pathological Classification • Preinvasive Neoplasia Esophageal intraepithelial neoplasia Glandular epithelial dysplasia/Adeno. CA in situ in Barrett's mucosa • Invasive Malignant Neoplasia Squamous cell carcinoma Adenocarcinoma, Adenoid cystic carcinoma Mucoepidermoid carcinoma Adenosquamous carcinoma Small cell carcinoma Carcinoid tumor Malignant melanoma & Sarcomas
AJCC TNM classification
Staging • TNM Stage • Tis N 0 M 0 Stage 0 • T 1 N 0 M 0 I • T 2 N 0 M 0 • T 3 N 0 M 0 IIA • T 1 N 1 M 0 • T 2 N 1 M 0 IIB • T 3 N 1 M 0 III • T 4 any N M 0 • Any T any N M 1 IV
Diagnostic Workup • Detailed history & Physical examination: • Confirmation of diagnosis: EGD: allow direct visualization and biopsy, measure proximal & distal distance of tumor from incisor, presence of Barrett’s esophagus. Early, superficial cancer Circumferential ulceration esophageal cancer Malignant stricture of esophagus
• Staging: CT chest and abdomen:
• Endoscopic Ultrasonography
• Barium swallow: – can delineate proximal and distal margins as well as TEF – Helpful for correlation with simulation film. • Rat tail appearance Bronchoscopy: rule-out fistula in midesophageal lesions. • Routine Investigations: CBC, chemistries, LFTs. Cancer lower 1/3 Filling defect (ulcerative type) Apple core appearance
• PET Scan: • most recently, proven to be valuable staging tool • can detect up to 15– 20% of metastases not seen on CT and EUS • low accuracy in detecting local nodal disease compared to CT / EUS • Value in evaluating response to Chemo Therapy & Radio Therapy
SURGICAL MEASURES Patients with esophageal CA are considered candidates for esophageal resection (1) there is no evidence of the spread of thetumor to structures next to the esophagus, such as the tracheobronchial tree, the aorta, or the recurrent laryngeal nerve; (2) there is no evidence of distant metastases; and (3) the patient is fit from a cardiac and respiratory point of view. An esophagectomy can be performed by using (1) an abdominal and a cervical incision with blunt dissection of the thoracic esophagus through the esophageal hiatus (transhiatal esophagectomy) or (2) an incision into the abdomen and the right side of the chest (transthoracic esophagectomy). After removing the esophagus, continuity of the gastrointestinal tract is reestablished by using either the stomach or the colon. The morbidity rate of the operation is approximately 30%
NONSURGICAL MEASURES • Neoadjuvant therapy based on a combination of radiation therapy and chemotherapy(5 FU, Cisplatin, Vinblastin, Leucovorin) has been attempted to improve both the local control, via radiation therapy, and the distant control of the disease, via chemotherapy. • . Nonoperative therapy is reserved for patients who are not candidates for surgery because of local invasion of the tumor, metastases, or a poor functional status. • The goal of therapy in these patients is palliation of the dysphagia, which will allow them to eat.
• The following treatment modalities are available to achieve this goal: • (1) Expandable, coated, metallic stents can be deployed by endoscopy under fluoroscopic guidance to keep the esophageal lumen open. • (2) Laser therapy (Nd: YAG laser) relieves dysphagia in up to 70% of patients. However, multiple sessions are usually required. • (3) Radiation therapy is successful in relieving dysphagia in about 50% of patients. • Prognosis • The overall 5 -year survival rate for esophageal cancer remains approximately 25– 30%.
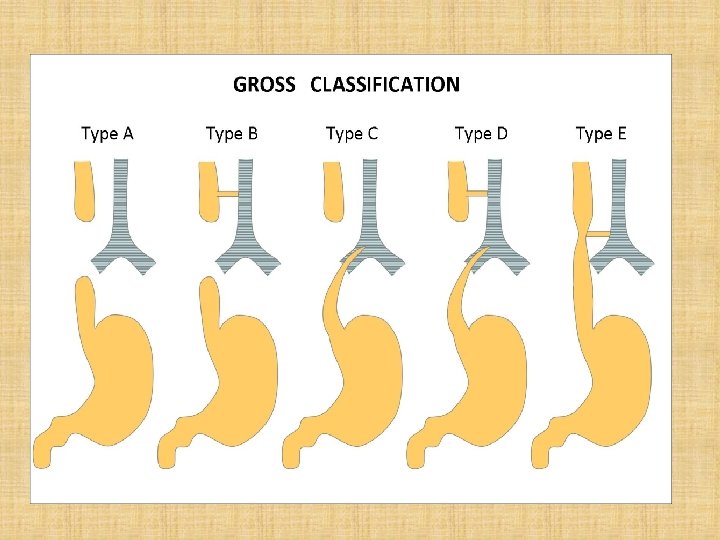
ESOPHAGEAL ATRESIA & TRACHEOESOPHAGEAL FISTULA • Prevalence 1 in 3000 live births, M=F. • Infants with these conditions are often premature, and polyhydramnios is commonly diagnosed prenatally. • Classification & Incidence: • • • Atresia with distal TEF 85. 4% Atresia without TEF 7. 3% TEF without atresia 2. 8% Atresia with proximal & distal TEF 2. 1% Atresia with proximal TEF < 1. 0%
References • Scott-Brown’s Otorhinolaryngolology, Head and Neck Surgery, Vol-2 , 7 th edition. • Cummings , Otorhinolarngology Head and Neck Surgery, Vol-2 , 4 th edition.