NICOTINE STOMATITIS SMOKERS PALATE STOMATITIS NICOTINA PALATI NICOTINE



 • Location- Hard palate posterior to")














 type like")


- Slides: 22
NICOTINE STOMATITIS / SMOKER’S PALATE/ STOMATITIS NICOTINA PALATI
NICOTINE STOMATITIS • Uncommon mucosal change of the hard palate as a result of cigar and pipe smoking • Develops in response to heat generated from smoking, not due to chemicals. • Not premalignant
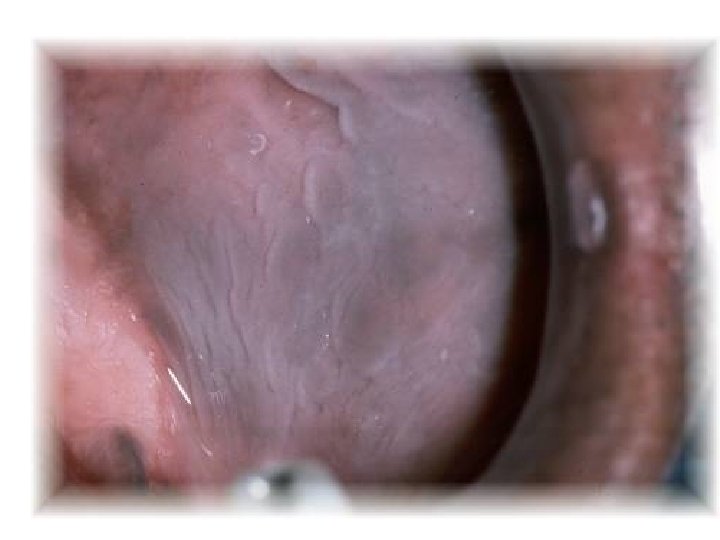
NICOTINE STOMATITIS
CLINICAL FEATURES • Older males (>40 -45 years) • Location- Hard palate posterior to rugae area • Begin as erythematous area that gradually thickens, becomes fissured and whitish gray. • Lesions show papular projections with red centers ( red centers representing inflamed orifices of minor salivary ducts)
Histopathologic features – Hyperkeratosis and acanthosis of epithelium – Chronic inflammation in the underlying connective tissue and mucous glands – Squamous metaplasia of the excretory ducts
Treatment and prognosis – Completely reversible following cessation of smoking – Mucosa returns to normal in 1 -2 weeks
Leukoedema • Condition of buccal mucosa which is a normal variation, may resemble early leukoplakia.
Etiology • Unknown • Use of tobacco, p. H of saliva, Oral bacterial infection, Syphilis & galvanism • Ethnic association also has been suggested
Clinical features • Varies from filmy opalescence of mucosa to more grayish white with coarsely wrinkled surface. • Bilaterally symmetrical and involve entire mucosa & even extending to labial mucosa • More distinct along occlusal plane& molar region • Surface may show erosions • Disappears on stretching the mucosa.
Histopathology • Increased thickening of epithelium • thick parakeratin layer Irregularly elongated broad rete ridges. • Intracellular edema of spinous cell layer • Edematous cells appear large & pale, cytoplasm appear lost, nucleus is pyknotic and give a reticular appearance.
Clinical significance & treatment • Variant of normal mucosa • No treatment required
SMOKELESS TOBACCO KERATOSIS • • Chewing tobacco: coarsely cut tobacco leaves Snuff: finely ground tobacco leaves Habit starts early in life (8 -14); rare after 20 Clinical findings – Loss of gingival and periodontal tissues – Gingival recession – Dental caries: high sugar content in products
Clinical findings – Halitosis – Staining of teeth – Keratosis • 15% of chewing tobacco users • 60% of snuff users • Young adult men • Takes 1 -5 years to develop
Clinical findings Takes 1 -5 years to develop Loss of gingival and periodontal tissues (Gingival recession) It is a white keratotic plaque, as is leukoplakia, but has a semitranslucent appearance rather than a flat whiteness • More wrinkled and more intensely white smokeless tobacco keratoses are considered to be "higher grade" lesions, • Those lesions remaining after two months without smokeless tobacco should be considered to be true leukoplakias, possibly developed from or hidden by the previous smokeless tobacco keratosis • • Dr. Maji Jose
Histopathologic features – Hyperkeratosis and acanthosis – Chevrons – Amorphous eosinophilic material in the connective tissue – Dysplasia is uncommon but may occur
Treatment and prognosis – Risk of developing carcinoma is 4 times greater than in nonusers • Squamous cell carcinoma > verrucous carcinoma – Cessation leads to normal mucosal appearance in 2 -6 weeks
TOBACCO POUCH KERATOSIS
• Metaplasia – Replacement of normal differentiated tissue by another (differentiated) type like epithelial to mesenchime transition in breast carcinoma progression • Anaplasia – Loss of differentiated phenotype • Dysplasia – Loss of tissue organisation • Hyperplasia – Increase in cell division
Neoplasia • Neoplasia - New growth • An abnormal mass of tissue, the growth of which exceeds and is uncoordinated with that of normal tissue and persists in the same excessive manner after cessation of the stimuli which evoke the change.
• Cancer – Any Malignacy • Carcinoma – Epithelial Malignancy • Sarcoma – Connective tissue Malignancy