Nicotine history and numbers probably 2 nd most

Nicotine � history and numbers ◦ probably 2 nd most widely used psychoactive drug in our society ◦ just another plant waiting to be discovered ◦ used long before Columbus arrived in the “new world”

Nicotine �History: No society that has adopted tobacco has ever given it up. �Only drug of abuse that is native to the Americas. ◦ Is widely speculated that tobacco has been cultivated in the Americas since 6, 000 B. C. �Given to Columbus when he landed at San Salvador on Oct. 12, 1492. ◦ Christopher Columbus and his crewman on their voyage to the "New World" were the first Europeans to see tobacco smoking.

� � formally introduced to Europe as a medicinal herb over 60 species of nicotiana but only 2 major ones;

Evolutionary strategy of plants � nicotine – ◦ potent poison and bitter flavor! � most bugs, etc will keep away from it! ◦ tobacco leaves contain up to 10% nicotine

Forms of tobacco � cigarettes – predominant form of tobacco used in US ◦ cigars, pipes, smokeless tobacco

Epidemiology and smoking � Nationwide – estimates of 51, 000 smokers with a large proportion considered dependent on nicotine � Nationwide- estimates of 25, 000 have tried cocaine but less than 1, 000 daily users

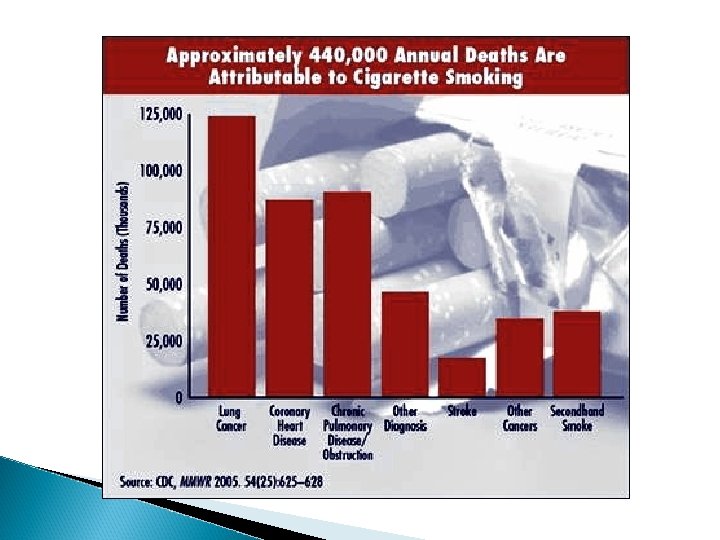
From the CDC, December 2009 � Cigarette smoking is the leading cause of preventable death in the United States, accounting for approximately 443, 000 deaths or 1 of every 5 deaths in the United States each year. � Estimated 46 million people or 20. 6% of all adults (aged 18 years and older) in the United States currently* smoke cigarettes. ◦ more common among men (23. 1%) than women (18. 3%).

Age 21. 4% of adults aged 18– 24 years 23. 7% of adults aged 25– 44 years 22. 6% of adults aged 45– 64 years 9. 3% of adults aged 65 years and older Race/Ethnicity 21. 3% of Blacks (non-Hispanic) 32. 4% of American Indians/Alaska Natives 9. 9% of Asians** 15. 8% of Hispanics By Education 22. 0% of Whites (non-Hispanic) 41. 3% of adults with a GED diploma 35. 7% of adults with 9– 11 years of education 10. 6% of adults with an undergraduate college degree 5. 7% of adults with a graduate college degree

State Estimates* Current smoking prevalence was highest in the following states: 5 Adults West Virginia 26. 6% Indiana 26. 1% Kentucky 25. 3% Men Indiana 28. 5% Missouri 27. 3% Tennessee 26. 7% Women West Virginia 27. 1% Kentucky 24. 3% Indiana 23. 9%

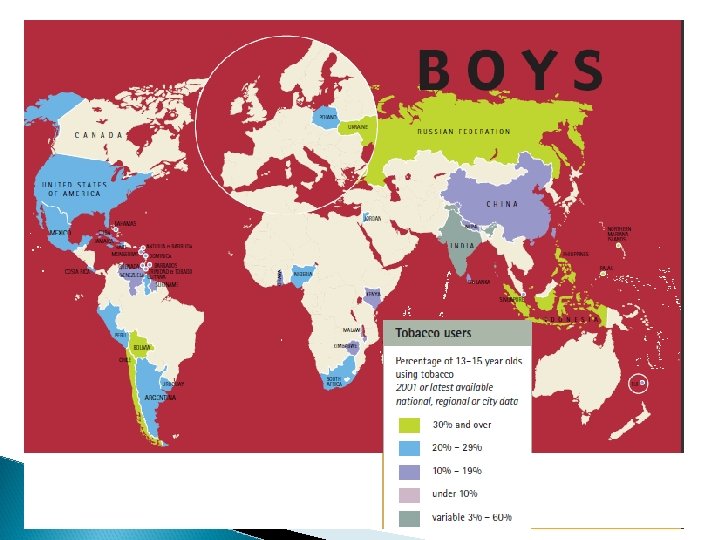
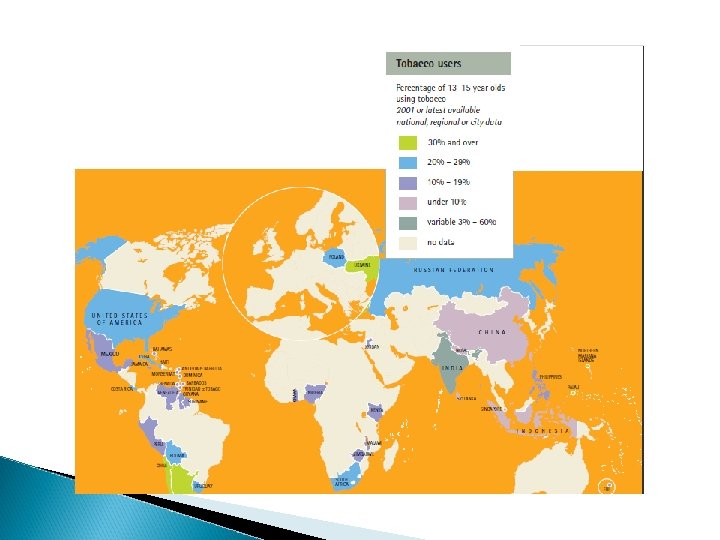
Youth smoking � Data from the WHO

How can we reduce youth smoking?

Health related cost �Nicotine dependence – ◦ stereotypic and compulsive patterns of behavior, ◦ positively and negatively reinforcing ◦ physical dependence �smoking or smokeless tobacco responsible for 400, 000 deaths/year (contrast with 6000 for heroin and cocaine combined)

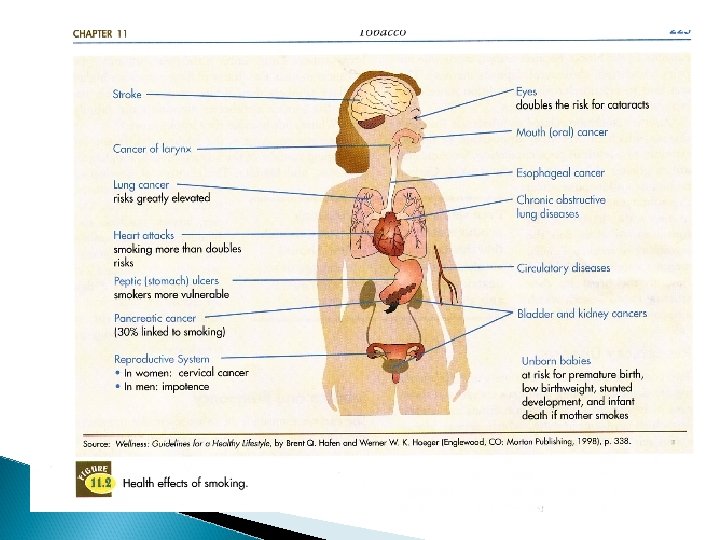
What are the major health risks?
 � classified by EPA as a known cause of lung")
2 ndhand smoke (cont) � classified by EPA as a known cause of lung cancer in humans � irritant to eyes, nose throat, � estimated ~ 3000 deaths/year to nonsmokers � infants and children at greatest risk for respiratory infections, ear infections, asthma ◦ (est that 200, 000 to 1 m asthmatic kids have condition made worse by 2 nd hand smoke – may increase risk of asthma as well)

Pharmacokinetics � absorption- ◦ inhalation – 90% inhaled nicotine is absorbed ◦ n average cigarette yields about 1 mg of absorbed nicotine ◦ one of the most toxic drugs known – 60 mg is lethal and death follows intake within a few minutes � � Symptoms: Abdominal pain, nausea, vomiting, diarrhea, headaches, decrease in blood pressure, death from suppression of breathing. Absorbed from every site on, or in, the body

Pharmacokinetics � absorption- ◦ one study found an average increase of 1. 6% per year between the years of 1998 and 2005. ◦ one of the most toxic drugs known – 60 mg is lethal and death follows intake within a few minutes ◦ cigars – contains enough nicotine for two lethal doses (burning destroys much of the nicotine)
 � mouth absorption")
� smoke of tobacco in most cigarettes is ionized (? ) � mouth absorption is very limited – need to inhale deeply to the highly vascularized lungs
 is alkaline (and nicotine")
� smoke of most pipes, cigars (and some European cigarettes) is alkaline (and nicotine is nonionized) � gum and snuff are also buffered so they are at a more alkaline p. H

� differences in how nicotine is absorbed contributes to the dependence potential ◦ inhalation – very rapid ◦ oral – more slowly but longer lasting

� nicotine is distributed very quickly � readily crosses the blood brain barrier � ~ 7 secs � ½ life is around 2 hours

Nicotine is quickly and thoroughly distributed in the body, to brain, placenta, all body fluids (including breast milk). � Liver metabolizes 80– 90 percent before excretion by kidneys. � Elimination half-life is ~2 hours. The major metabolite of nicotine is cotinine, which is basis for tests. �
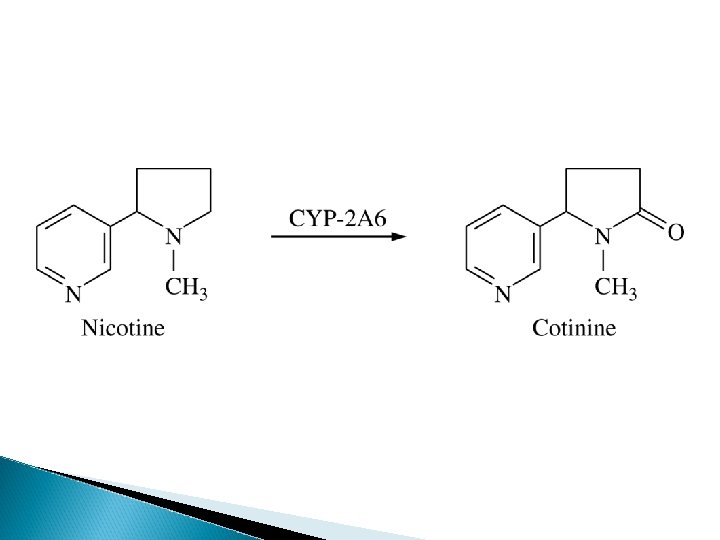

Metabolism � Enzymes in the CYP 450 family ◦ (mostly CYP 2 A 6, also CYP 2 B 6 ◦ A major metabolite is cotinine.

All psychoactive effects are most likely due to nicotine – some of the more carcinogenic effects are due to how we get nicotine into our body.

What are the behavioral effects of nicotine? � rewarding, ◦ how? pleasurable effects � paradoxical effects on arousal ◦ biphasic effect with increased attention at lower doses but decreased anxiety/arousal at higher doses � decreased reduction hunger and resulting weight ◦ nt release and increased metabolism because of sympathetic NS activation

How does nicotine exert behavioral effects? � n. ACh receptors – nicotinic subtype of ACh receptors � at least 17 subtypes now recognized

4 families of nicotinic receptors

How does nicotine exert behavioral effects? � n. ACh receptors – nicotinic subtype of ACh receptors � where ◦ PNS are these receptors found? �autonomic ns �neuromuscular junction

How does nicotine exert behavioral effects? �n. ACh receptors – nicotinic subtype of ACh receptors ◦ fast onset; short duration; excitatory �where ◦ PNS are these receptors found? �autonomic ns �neuromuscular junction �biphasic effect ◦ low dose – stimulation; high dose – brief stimulation followed by blockade of transmission

CNS ACh nicotinic receptors � found � some in hippocampus n. ACh. R are presynaptic and when bound may enhance excitatory input to DA neurons in reward areas

Nicotine Pharmacological effects Initially causes nausea and vomiting by stimulating vomiting center in brain stem and sensory endings in stomach. This becomes tolerant. � Stimulates hypothalamus to produce antidiuretic hormone, causing fluid retention. � Reduces activity coming in from muscles, producing relaxation. � Increases heart rate, blood pressure and contractility; but carbon monoxide in smoke combines with oxygen better than hemoglobin, so it decreases oxygen carrying capacity (suffocates cells). �

Nicotine also � stimulates release of catecholamines, stress hormones, adrenaline, epinephrine, etc. .
. � Inhibits")
Nicotine Constricts blood vessels in skin, producing cold, thin, wrinkles (faster aging). � Inhibits stomach secretions, stimulates bowel (laxative in nontolerant person). � May increase metabolism of fat; dull taste buds. � Slows stomach contractions; increases blood sugar. � May improve attention/memory; although high doses may increase nervousness, tremors, seizures, panic attack. � May have an antidepressant effect (i. e. , are smokers self-medicating? ). �

Nicotine Nesbitt’s paradox: Nicotine causes arousal and a release of epinephrine, yet most people say it relaxes them. This may be relevant to the reason people smoke. Is it simply relief from withdrawal? Does it depend on the stress of the situation? (Relaxation with high stress, stimulation with low? ) Smokers report positive subjective effects if nicotine is given by smoking or intravenously, but nonsmokers do not like it.

Does tolerance develop? � first smoking experience � overnight � low abstinence nicotine cigarettes and behavior
 ◦ reduces risk of Parkinson’s disease")
Believe it! �smoking (almost certainly due to nicotine) ◦ reduces risk of Parkinson’s disease ◦ reduces risk of Alzheimers �schizophrenics on neuroleptics smoke in very large numbers – why? �nicotine also can ◦ be neuroprotective (against ETOH WD neurotoxicity for example) ◦ suppress certain autoimmune diseases

What about animal models? � nicotine self-administration � smoking � primates chambers

Smoking cessation � most surveys show that the majority of smokers want to quit……. � behavioral therapies may be important � pharmacotherapy may be important � neither of these (alone or together) is enough for most!

Why is it so hard? � psychological dependence � physical dependence vs physical withdrawal signs ◦ lower heart rate, tremors, headaches, anxiety, shorter attention span, insomnia, increased appetite, etc…. � Psychological dependence

Pharmacotherapies � substitution and weaning

Pharmacotherapies � substitution and weaning ◦ nicotine patch, ◦ nicotine gum ◦ nicotine inhaler – approved in 1996
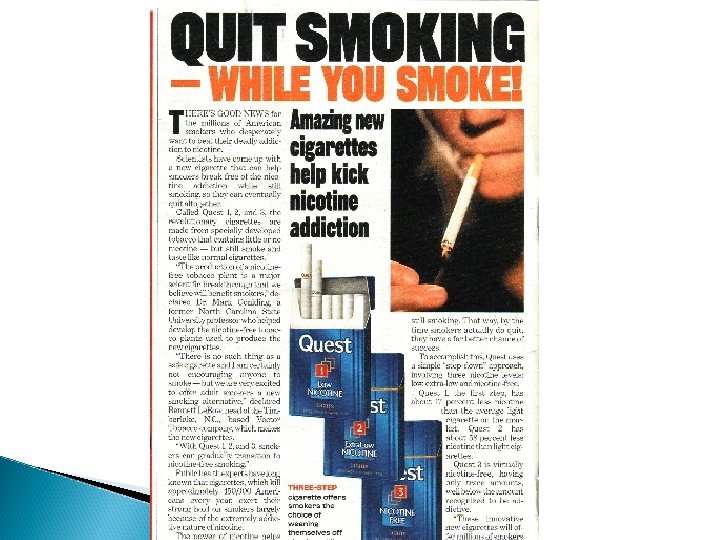

Figure 14. 8 Plasma nicotine levels Julien: A Primer of Drug Action, Eleventh Edition
 – approved in 1997 for smoking cessation")
Pharmacotherapies � other drugs ◦ Zyban (buproprion) – approved in 1997 for smoking cessation �originally an antidepressant (Wellbutrin) �mechanism of action not well understood �weak inhibitor of dopamine and noradrenaline reuptake, and has also been shown to antagonize nicotinic acetylcholine receptor function.
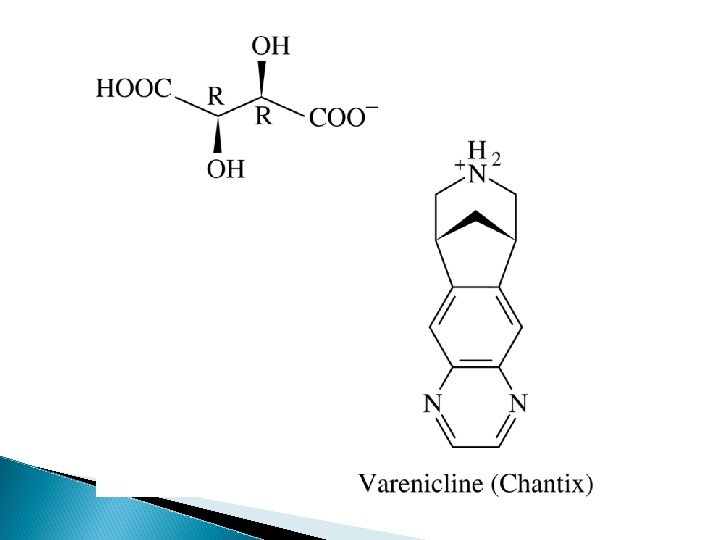

How does varenicline work? � partial agonist/antagonist � alpha 4/beta 2
- Slides: 51