Frequency of Adverse Events Following Primary Smallpox Vaccination





 ulcers")















- Slides: 25
Frequency of Adverse Events Following Primary Smallpox Vaccination with New York Board of Health Strain Vaccinia, by Age and Type of Adverse Event Expected Number of Adverse Events Per Million Vaccines Age at Vaccination <1 1 -4 5 -19 20+ Death (all causes) 5 0 -5 5 (? ) Post-vaccinial encephalitis 6 2 3 4 Progressive vaccinia 1 0. 5 1 10 + (? ) Eczema vaccinatum 14 44 35 30 Generalized rashes 400 9, 600 140 250 Accidental implantation 507 577 371 606 Type of Adverse Event
What is Herpes? Herpes is a common viral infection. It causes oral herpes (cold sores or fever blisters), and genital herpes (genital sores). There are two herpes simplex viruses: • Herpes Simplex Type 1 (HSV-1) • Herpes Simplex Type 2 (HSV-2) These viruses look identical under the microscope, and either type can infect the mouth or genitals. Most commonly, however, HSV-1 occurs above the waist, and HSV-2 below.
GENITAL HERPES Genital herpes is a contagious viral infection affecting primarily the genitals of men and women. It is characterized by recurrent clusters of vesicles and lesions at the genital areas. It is caused by the Herpes Simplex-2 virus (HSV-2), one of several strains of the Herpes Simplex Virus responsible for chickenpox, shingles, mononucleosis, and oral herpes (fever blisters or cold sores, HSV-1). While generally not dangerous, it is a nuisance and can be emotionally traumatic, as there is no cure. It has reached epidemic proportions in the U. S. ; 500, 000 are diagnosed each year. One in five American adults has herpes, but only one third of those inflicted are aware that they have the virus. Many people don’t relate their symptoms to herpes, since they have either very mild or no symptoms at all. Over 50 million cases are currently estimated to exist in either the active or dormant stage.
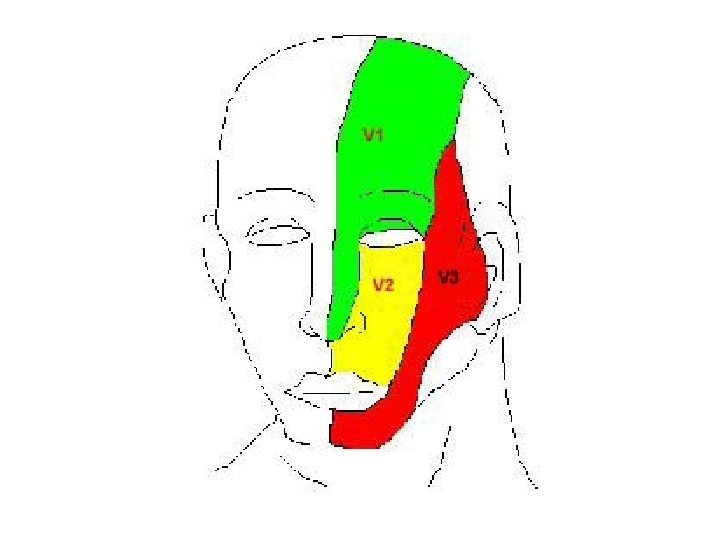
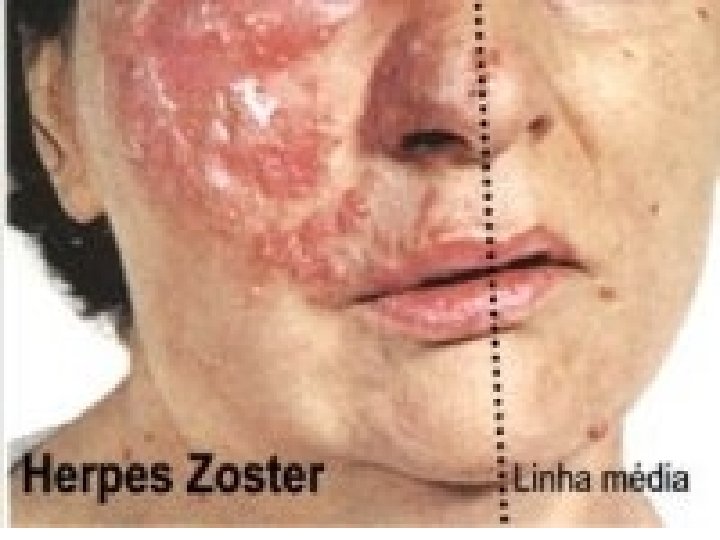
The hallmark of herpes zoster ophthalmicus is a vesicular rash that involves the first (ophthalmic) division of the fifth cranial nerve that presents in a dermatomal distribution and respects the midline (a). The upper eyelid is commonly involved with edema, inflammation, and resultant ptosis (b). The sensory distribution of the ophthalmic (V ) division of the trigeminal nerve (c, d)
• Groups of vesicles arranged along the distribution of a cranial or spinal nerve • Cutaneous and visceral dissemination from the original dermatome develops in some individuals, particularly immunocompromised patients • Associated with localized or referred pain
Eczema herpeticum (ulcers are of similar shape and size) ulcers
“The key physical sign of eczema herpeticum is blisters, pustules, or erosions of a rather uniform size and appearance”
Definition: Eczema vaccinatum is a serious complication that occurs when people with eczema or atopic dermatitis get vaccinated. The lesion spreads to skin that is currently affected or has recently been affected by eczema. This complication can occur even if the eczema or atopic dermatitis is not active at the time, and requires immediate medical attention. Prior to 1960, eczema vaccinatum occurred in 10 to 39 people per 1 million people vaccinated. Vaccine Immune Globulin (VIG) is felt to be a useful treatment for eczema vaccinatum.
Eczema vaccinatum is characterized by widespread vaccinial lesions over the body of patients with eczema or a history of eczema. These patients are clinically similar to burn patients, losing fluid, serous exudate, and electrolytes through their skin. Fatalities often occurred in patients who were not themselves vaccinated, but were close household contacts of recently vaccinated siblings etc. Many patients with eczema have perfectly normal vaccination responses; there are no data to show what proportion of eczema patients develop serious disease, but it is probably considerably less than half. While patients with other widespread skin disease can get superinfection of their rashes, they do not develop the extensive involvement found with occasional eczema patients, and essentially never die. Vigorous therapy with VIG and good supportive care reduced the fatality rate from about 10% in the pre-VIG era, to only about 1%.
Eczema vaccinatum • Eczema vaccinatum is a localized or systemic spread of vaccinia virus. • In the past, it was estimated to occur in 10 -39 per million primary vaccinees. * Rates in the United States today may be higher because there may be more persons at risk from 1) immune suppression from cancer, cancer therapy, organ transplantation, and other illnesses, such as HIV/AIDS, and 2) eczema or atopic dermatitis. Rates may be lower for persons previously vaccinated • Transfer of vaccinia virus can occur from autoinoculation or from contact with a vaccinee whose lesion is in the florid stages. • Individuals with eczema or atopic dermatitis are at increased risk. Eczema vaccinatum can occur regardless of whether the eczema/atopic dermatitis is active at the time of vaccination. • Virus implanted in disrupted skin (may be at multiple sites) spreads from cell to cell producing extensive lesions dependent on extent of abnormal skin. • Treatment should include hospitalization and urgent treatment with VIG. Mortality has been prevented in patients treated promptly and adequately. • Severe cases and fatalities have been observed after contact of recently vaccinated persons with persons who have active eczema/atopic dermatitis or a history of eczema/atopic dermatitis.
Eczema vaccinatum.
Eczema vaccinatum.
Eczema vaccinatum in contact to recently vaccinated child. Recovered without sequelae or permanent ocular damage.
Eczema vaccinatum in an unvaccinated contact to a vaccinated sibling. [from Fenner F. , Henderson DA, et al. Smallpox and its Eradication. WHO. 1988].
Generalized vaccinia • Generalized vaccinia consists of vesicles or pustules appearing on normal skin distant from the vaccination site. • In the past, it was estimated to occur in 242 per million primary vaccinees. • It is believed to result from a vaccinia viremia with skin manifestations. • Most rashes labeled as generalized vaccinia produce only minor illness with little residual damage. • The rash is generally self-limited and usually requires only supportive therapy. However, patients with underlying immunosuppressed illnesses may have a toxic course and require Vaccinia Immune Globulin (VIG).
Generalized vaccinia in an apparently normal child. Recovered without sequelae.
Generalized vaccinia This child touched his inoculation site and inoculated his lower lid with vaccinia virus. More common, but of less concern are accidental implantations, erythematous or urticarial rashes, and “generalized vaccinia. ” Accidental implantation occurs when a patient scratches his/her vaccination site, and then scratches an eye, the anus or genitals, or another skin disorder such as poison ivy. This creates a coprimary lesion distant from the intended vaccination site. When vaccinia infects the eye, care must be taken to examine for keratitis. About 6% of patients with vaccinia in the eye develop vaccinial keratitis; VIG is contraindicated in such patients, because they may get antigen-antibody precipitates in the cornea causing scarring. Widespread blotchy macular rashes, often with dramatic erythema and/or urticaria, are very common, especially in toddlers. These may worry the parents considerably, but the patients do very well with no therapy. Rarely a true Stevens-Johnson-like rash occurs which requires more vigorous medical intervention. There is a blurry spectrum of these rashes, many of which are labeled “generalized vaccinia”. This term implies that the vaccinia virus has become bloodborne and spread throughout the body. The erythematous/urticarial rashes do not have virus replication in peripheral lesions; true generalization of the virus with virus-containing peripheral pustules is fairly uncommon.
Inadvertent Inoculation • Successful vaccination produces a lesion at the vaccination site. Beginning about four days after vaccination, the florid site contains high titers of vaccinia virus. This surface is easily transferred to the hands and to fomites, especially since itching is a common part of the local reaction. • Accidental implantation occurs due to transfer of vaccinia virus from the primary site to other parts of the body, or to other individuals. • This is the most frequent complication of smallpox vaccination (529 per million primary vaccinees), accounting for approximately half of all complications of primary vaccination and revaccination. • Lesions of inadvertent inoculation can occur anywhere on the body, but the most common sites are the face, eyelid, nose, mouth, genitalia, and rectum. Lesions in eczematous skin, in disrupted skin and in the eye pose special hazards, as the infection can be extensive in skin lesions and a threat to eyesight in the eye. • Most lesions heal without specific treatment
Vaccinia keratitis • Vaccinia keratitis results in lesions of the cornea due to accidental implantation of vaccinia virus, and is potentially threatening to eyesight. • Symptoms appear ten days after transfer of vaccinia virus. • Left untreated, considerable corneal scarring may result as lesion heals resulting in significant impairment of vision. • Topical antiviral agents are the treatment of choice; therapy should be determined in immediate consultation with an experienced ophthalmologist.
Progressive vaccinia • Progressive vaccinia, also known as vaccinia necrosum, is a severe, potentially fatal illness characterized by progressive necrosis in the area of vaccination, often with metastatic lesions (e. g. , lesions at places other than the vaccination site). • In the past, it was estimated that progressive vaccinia occurred in approximately 1 to 2 per million primary vaccinations, and was almost always fatal before the introduction of VIG and antiviral agents. • Rare in the past, it may be a greater threat today, given the larger proportion of susceptible persons in the population and the greater number with immunocompromise. Nearly all instances have been in people with defined cell-mediated immune defect (T-cell deficiency). • Prompt hospitalization and aggressive use of VIG are required. • Massive doses of VIG are necessary to control viremia. Up to 10 ml per kg of intramuscular VIG has been used. • There is no proven antiviral therapy. Preliminary studies with cidofovir show some antiviral effect in vitro; studies in animals are pending. • Immediate consultation with the CDC is recommended to determine if any experimental antiviral drugs are available.
Electronic sources of dermatological information Dermatology Online Journal tray. dermatology. uiowa. edu/home. html Internet Dermatology Society Rx. Derm-L Tumours of the skin, University of California at Davis Dermatology online atlas Dermatology atlas www. telemedicine. org listpro@ucdavis. edu (email) matrix. ucdavis. edu/tumors/tradition/tumors. html www. derma. med. unierlangen. de/index_e. htm www. meddean. luc. edu/lumen/med. Ed/medici ne/dermatology/melton/atlas. htm Skin cancer and benign tumor image atlas www. meddean. luc. edu/lumen/med. Ed/medici ne/dermatology/content. htm Dermatology image bank www. tmc. edu. tw/medimage/derma_bank/de fault_eng. htm www. telemedicine. org/contact. htm www. dermnet. org. nz/dna 2 a. html erl. pathology. iupui. edu/cases/dermcases/der mcases. cfm www. skindex. Contact dermatitis Derm. Net (atlas and information) Virtual Dermatology (case directory) Skindex-case directory (news, reviews, treatment trends, meeting reports, CME, case reports, disease descriptions, atlas, Q&A site)