Food Allergies Fatemeh Sedaghat Ph D in Nutrition


















![Summary of 2008 AAP Guidelines for Allergy Management [Greer et al 2008] l There](https://slidetodoc.com/presentation_image_h2/0f90fa4b61263a36474bf7773b6c8b77/image-20.jpg "Summary of 2008 AAP Guidelines for Allergy Management [Greer et al 2008] l There")



 recommended avoidance of")





- Slides: 30
Food Allergies Fatemeh Sedaghat Ph. D in Nutrition Sciences Shahid Beheshti Medical University 11/2019
Discussion Topics l l l l What is a food allergy? Who gets a food allergy? Most common food allergies Symptoms How is it diagnosed? How can you avoid food allergies? Tips to prevent allergies
What Is a Food Allergy? l l l Immune system function Super-sensitive Allergens (Usually the protein part) Allergens react to antibodies Release chemicals causing symptoms
What Is The Difference Between Food Allergy and Food Intolerance? l Food allergy causes an immune system response, causing symptoms in your child that range from uncomfortable to lifethreatening. l Food intolerance does not affect the immune system, although some symptoms may be the same as in food allergy.
Food Intolerance l l l l More common than allergies Food poisoning Histamine toxicity (cheese, wine, fish) Lactose intolerance Food additives (MSG) Gluten intolerance (small intestine) Corn products
What is the difference between food allergy and food intolerance?
Who Gets a Food Allergy? l Prevalence of food allergy highest in infants and toddlers. l About 3 to 8 percent of children have food allergies. l About 1 to 2 percent of adults.
Who Gets a Food Allergy? l It was previously thought that most children would "outgrow" their food allergies by 4 years of age; however, it is becoming apparent that this is not the case. l Only 11% of egg-allergic and 19% of milk-allergic children resolved their allergies by 4 years of age. However, almost 80% resolved these allergies by age 16. l This is not true for peanut allergy, which is considered a persistent allergy lasting a lifetime for most children.
Most Common Food Allergies l Children l l l Milk, egg, peanuts, wheat, soy, tree nuts Most will outgrow eggs, milk, wheat, and soy Adults l Peanuts, tree nuts (almonds, walnuts), fish, shellfish (shrimp, lobster, crab), mollusks (oysters, clams, scallops)
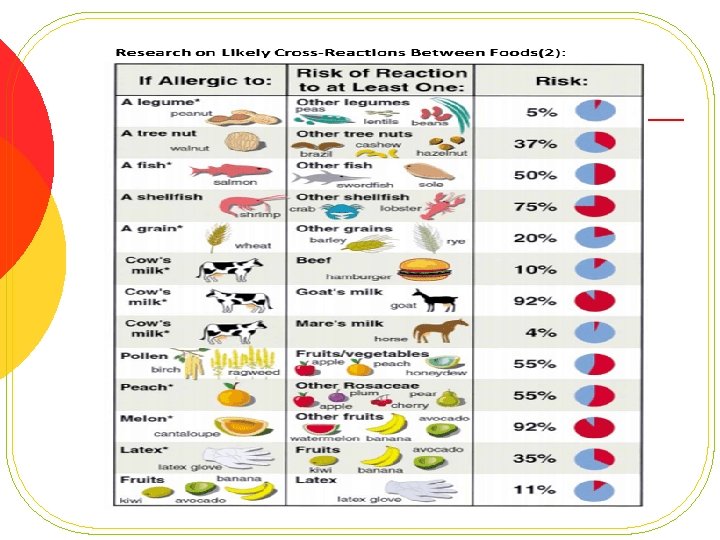
If Allergic to One Food, Do You Have to Avoid Related Foods? l Cross-reactivity occurs when the proteins in one substance are like the proteins in another. As a result, the immune system sees them as the same. l In the case of food allergies, cross-reactivity can occur between one food another. Crossreactivity can also happen between pollen and foods or latex and foods.
Symptoms of Food Allergies l Reaction within minutes to two hours. l How soon and how severe depend on sensitivity to food, how much was consumed, other foods consume, and preparation. l May have minor symptoms at first.
Symptoms l Digestive system l l l l Swelling, itching Tightness Hoarseness Nausea Cramping Pain Vomiting Diarrhea l Body systems (skin, lungs, etc) l l l Hives, skin swelling Anaphylaxis – BP falls, wheezing, breathing problems, nausea, rapid pulse, flushing, faintness, passing out Can lead to death
Symptoms l l l Severe reactions more common in peanuts, tree nuts, shellfish, and eggs. Also more common in those with asthma. Death usually seen in peanuts or tree nuts.
Milk and soy allergy symptoms l Allergies to milk and soy are usually seen in infants and young children. l Often, these symptoms are unlike the symptoms of other allergies, but, rather, may include the following: l Colic (fussy baby) Blood in your child's stool Poor growth l l
How are food allergies diagnosed? l l l l Physician Medical history, physical exam Skin test Lab tests Oral food challenge Elimination diet Double-blind food challenge
Prevention of Food Allergies l The development of food allergies cannot be prevented, but can often be delayed in infants by following these recommendations: l If possible, breastfeed your infant for the first six months. l Do not give solid foods until your child is 6 months of age or older. l Continue to breastfeed complementary foods. whilst introducing
Prevention of Food Allergy in Clinical Practice Significant change in directives within the past 5 years: l Previously: Avoidance of allergen to prevent sensitization (allergen-specific Ig. E). l Current: Active stimulation of the immature immune system to induce tolerance of antigens in food.
Significance in Practice l Food proteins demonstrated to cross the placenta and can be detected in amniotic fluid. l Exposure to small quantities of food antigens from mother’s diet thought to tolerize the fetus, by means of Ig. G 1 and Ig. G 3, within a “protected environment”.
Summary of 2008 AAP Guidelines for Allergy Management [Greer et al 2008] l There is no convincing evidence that women who avoid highly allergenic foods, or other foods during pregnancy and breast-feeding lower their child’s risk of allergies. l For high-risk for allergy infants (one first-degree relative with established allergy), exclusive breastfeeding for at least 4 months prevents or delays the occurrence of atopic dermatitis (eczema), cow’s milk allergy, and wheezing in early childhood.
Summary of 2008 AAP Guidelines continued l In infants at high risk for allergy who are not exclusively breast-fed for 4 -6 months there is modest evidence that the onset of atopic disease (allergy), especially eczema, may be delayed or prevented by the use of hydrolyzed formulas. l There is no good evidence that soy-based infant formulas have any preventive effect on the development of allergy.
Infant Formulae for the Allergic Baby Current Recommendations l Cow’s milk based formula if there are no signs of milk allergy. l Partially hydrolysed (p. HF) whey-based formula if there are no signs of milk allergy in high risk for allergy group. l Extensively hydrolysed (e. HF) casein based formula if milk allergy is proven. Greer et al AAP 2008 Von Berg et al 2007
Recommendations for Introduction of Solids to High Risk for Allergy Infants l Little evidence that delaying the introduction of complementary foods beyond 4 -6 months of age prevents allergy. l Foods should be introduced one at a time in small amounts. l Mixed foods containing various potential food allergens should not be given unless tolerance to each ingredient has been assessed. l Wait on foods with common allergens l l l Cow milk – age 1 Eggs – age 2 Peanuts, nuts or fish – age 3 or after
Introduction of Peanuts l Directives from pediatric societies (1998 - 2007) recommended avoidance of peanuts by mothers during pregnancy and lactation, and delaying introduction of peanuts until after 2 or even 3 years of age. l Research indicates that incidence of peanut allergy in children rose dramatically in the years following release of these directives. l Recent research suggests: l Avoidance tolerance. of peanuts reduced development of l Early exposure leads to reduced incidence of peanut allergy.
Introduction of Fish l Historically, fish consumption during infancy was considered to be a risk factor for allergy. l Recent research indicates otherwise: l Regular fish consumption during the first year of life associated with a reduced risk for allergic disease by age 4 years (n=4089)1 l Babies of mothers who frequently consumed fish (2 -3 times per week or more) during pregnancy had one third less food sensitivities than those whose mothers did not consume fish during pregnancy 2 l 1 Kull l 2 Calvani et al 2006
Probiotics and Allergy Prevention l Probiotics and prebiotics may change the colonic microflora of the neonate. l Theory: l Non-allergic children have a predominance of lactobacilli and bifidobacteria. l Atopic children tend to have more clostridia and lower levels of bifidobacteria. l Probiotics could be used to change the “atopic” to a more “non-atopic flora”.
Current Status of Probiotics in Allergy Prevention l Beneficial effects of probiotic therapy depends on: l l l Type of bacteria selected Dosage of the bacteria delivered to the digestive tract Method of delivery of the bacteria to the GI tract (in formulae; in cereals) Age of the individual Length of duration of delivery Conclusion at the current state of research: l Probiotics cannot be recommended primary prevention of atopic disease generally for
Take Home Message l Allergy prevention emphasizes inducing tolerance rather than avoiding sensitization. l Beginning of tolerance to foods may occur in utero or during breast-feeding. l Restriction of maternal diet to avoid highly allergenic foods during pregnancy or lactation is contraindicated. l Unless either mother or baby is allergic to them.
Take Home Message l Management includes: l l l of established food allergy Accurate identification of the allergenic food(s). Careful avoidance of the food allergens– especially if there is any risk of anaphylaxis. Avoidance of unnecessary food restrictions.