Diabetes Selfmanagement Education Sara Sedaghat M D Gabric

Diabetes Self-management Education Sara Sedaghat, M. D. Gabric Diabetes Education Association August 2017

The History beyond Diabetes Education Joslin stated that Bouchardat was the first clinician to introduce patient education, including self‐monitoring of urine glucose Joslin E P (1952) Apollinaire Bouchardat. Diabetes 1: 490‐ 491 Apollinaire Bouchardat

The History beyond Diabetes Education Apollinaire Bouchardat 1806 -1886 “this daily measurement of glucosuria guides patients like the compass that guides the sailor on unknown oceans” Bouchardat A (1883) De la glycosurie ou Diabète sucré son traitement hygiénique. Libraire Germer Baillière, Paris
. \"Diabetes education: a global perspective. \" Practical Diabetes 32(6): 212.")
Chaney, D. (2015). "Diabetes education: a global perspective. " Practical Diabetes 32(6): 212.

Research Trend in Diabetes Education

Paradigm Shift in Diabetes Education More than 95% of diabetes care is done by the patient. (Funnell and Anderson 2000)

Paradigm Shift in Diabetes Education Traditional knowledge-based diabetes education is essential but not sufficient for sustained behavior change. (Piette, Weinberger, Mc. Phee, 2000)

Paradigm Shift in Diabetes Education • Outcome-driven practice Outcome-driven • Patient-centered goals Patient-centered • Facilitating behavior change AADE (2014). "AADE 7 Self-Care Behaviors AADE Position Statement. "
 Diabetes self-management education (DSME) is the ) ongoing process of")
Diabetes Self-management Education (DSME) Diabetes self-management education (DSME) is the ) ongoing process of ongoing process facilitating the knowledge, skill, and facilitating ability necessary for diabetes self-care (Powers, Bardsley et al. 2017)
 On‐going support is critical to sustain progress made by participants")
Diabetes self-management Support (DSMS) On‐going support is critical to sustain progress made by participants during the DSME program. (Norris, Lau, Smith, Schmid, Engelgau. 2002) (Skinner. Cradock. Arundel, Graham. 2003) (Powers, Bardsley et al. 2017)

Ongoing DSMS Activities that assist the person with diabetes in implementing and sustaining the behaviors needed to manage his or her condition on an ongoing basis. The type of support provided can be behavioral, educational, psychosocial, or clinical (Powers, Bardsley et al. 2017)

Patient Education Vs DSME • Both are necessary • Patient Education: simple transfer of information • DSME encompasses the complex array of knowledge, skills, and abilities needed to maximize effective self‐ management. (Burke, Sherr et al. 2014)

What Is the Framework for Diabetes Education?

Patient-Centered DSME: AADE 7 Self-Care Behaviors 1. 2. 3. 4. 5. 6. 7. Healthy Eating Being Active Monitoring Taking Medications Problem Solving Healthy Coping Reducing Risk AADE (2014). "AADE 7 Self‐Care Behaviors AADE Position Statement. "
. \"AADE 7 Self-Care Behaviors AADE Position Statement. \"")
DSME Outcome Continuum AADE (2014). "AADE 7 Self-Care Behaviors AADE Position Statement. "

DSME Benefits • Hb A 1 C • Diabetes complications • Quality of life • Lifestyle behaviors • Coping • Health care costs (Powers, Bardsley et al. 2017)
")
DSME & Glycemic control (Chrvala, Sherr et al. 2016)
")
(Chrvala, Sherr et al. 2016)

DSME & Glycemic control • 118 unique interventions • 61. 9% reporting significant changes in A 1 C • Overall mean reduction in A 1 C was 0. 74 and 0. 17 for intervention and control groups • An average absolute reduction in A 1 C of 0. 57 (Chrvala, Sherr et al. 2016)
")
Mode of DSME Delivery (Chrvala, Sherr et al. 2016)
")
Effect of Baseline Hb. A 1 c (Chrvala, Sherr et al. 2016)

DSME Contact Time
")
Group Base Education (Odgers‐Jewell, Ball et al. 2017)

Group-based Education Advantages • Reduced time • Time for the provision of more detailed information • Decreased time demands on health workers • Easy incorporation of families and care givers • Facilitation of discussions and support from others facing the same challenges
")
(Odgers‐Jewell, Ball et al. 2017)

Primary outcome • Hb. A 1 c • Group‐based intervention was effective in reducing Hb. A 1 c by 0. 3% • Statistically significant improvements at 6– 10, 12 – 14, 18 and 36– 48 months, but unexpectedly, not at 24 months post intervention
")
(Odgers‐Jewell, Ball et al. 2017)

Group‐based intervention was effective in reducing Hb. A 1 c by 0. 3% (Odgers‐Jewell, Ball et al. 2017)

Physician‐, dietitian‐ and nurse‐led group‐based education interventions were equally effective at improving Hb. A 1 c levels. (Odgers‐Jewell, Ball et al. 2017)

Peer Support • Use of peer facilitators complementing health professionals, rather than replacing them. • Role modeling • Ongoing support: practical and emotional • Non‐hierarchical and reciprocal relationship (Odgers‐Jewell, Ball et al. 2017)

Patient-Centered DSME: AADE 7 Self-Care Behaviors 1. 2. 3. 4. 5. 6. 7. Healthy Eating Being Active Monitoring Taking Medications More researches on all aspects! Problem Solving Healthy Coping Reducing Risk AADE (2014). "AADE 7 Self‐Care Behaviors AADE Position Statement. "
 DAFNE: • DESMOND: Diabetes")
Structured DSME • DAFNE: Dose Adjustment for Normal Eating (DAFNE) DAFNE: • DESMOND: Diabetes Education and Self Management for DESMOND: Ongoing and Newly Diagnosed • DAFYDD: Dose Adjustment for your Daily Diet DAFYDD: • BERTIE: Beta Cell Education Resources for Training in Insulin and BERTIE: Eating • ASPIRE: Skills Programme matching Insulin Requirements to ASPIRE: Eating & Exercise • PRISMA • X-PERT

Psychologist GP Internist / Endocrinologist Patient Diabetes Specialist Nurse Dietician
")
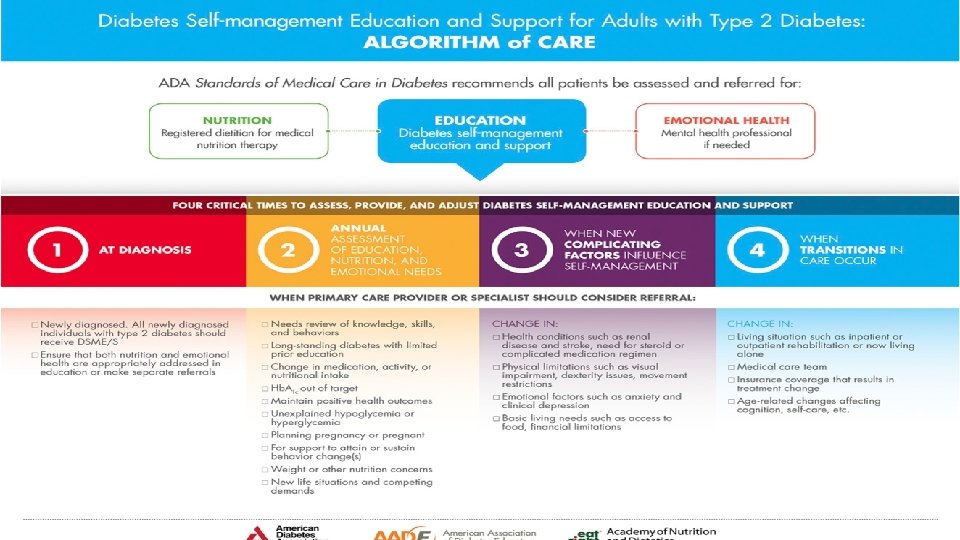
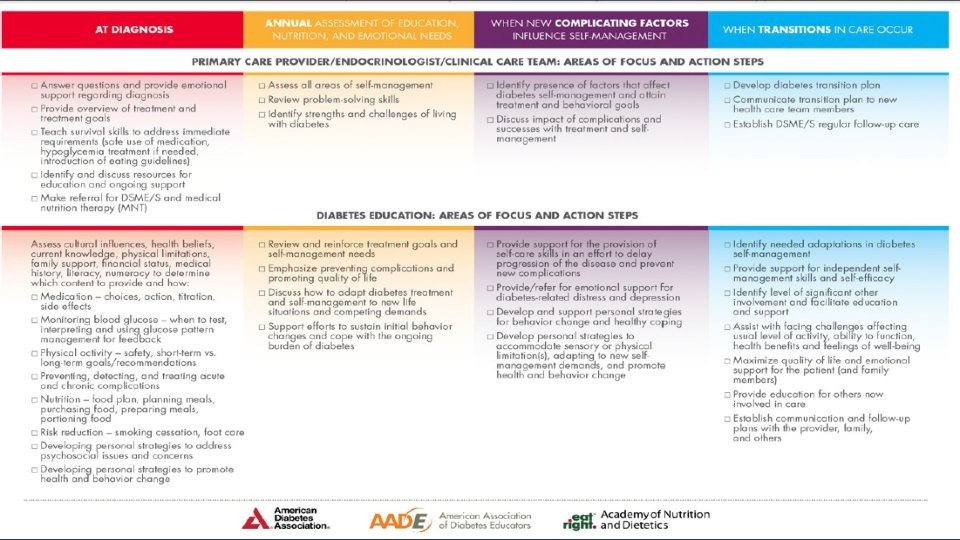
When we should provide DSME/S? (Powers, Bardsley et al. 2017)

Who Should deliver DSMES to the person with Diabetes?

Diabetes Educator • The effectiveness of the various disciplines for education are mixed. • Registered nurses, registered dietitians, and registered pharmacists Educators, AADE (2009). "AADE Guidelines for the Practice of Diabetes Self‐Management Education and Training (DSME/T). " The Diabetes Educator 35(3_suppl): 85 S‐ 107 S.

• Level 1: Non–Health Care Professional • Level 2: Health Care Professional /Non diabetes Educator • Level 3: Non credentialed Diabetes Educator • Level 4: Credentialed Diabetes Educator • Level 5: Advanced Level Diabetes Educator/ Clinical Manager Educators, AADE (2009). "AADE Guidelines for the Practice of Diabetes Self‐Management Education and Training (DSME/T). " The Diabetes Educator 35(3_suppl): 85 S‐ 107 S.

Diabetes Educator In‐depth knowledge and skills derived from the biological and social sciences, communication, counseling, and education Extensive knowledge of diabetes management Self‐management goals improvements in: • Clinical outcomes • Problem‐solving skills • Perception of overall health status • Quality of life

The diabetes educator is in a unique position to address patients and health care system needs. Educators, AADE (2009). "AADE Guidelines for the Practice of Diabetes Self‐Management Education and Training (DSME/T). " The Diabetes Educator 35(3_suppl): 85 S‐ 107 S.

The Real challenge is…… Low Utilization of DSME/S despite its proven benefits (Li, Shrestha et al. 2014)
")
Access to Diabetes Self-management Education (Peyrot and Rubin 2008)
")
Barriers to DSME Use (Peyrot and Rubin 2008)
")
Barriers to DSME Use (Peyrot and Rubin 2008)
")
Educator and Physician Recognition of Patient Barriers to DSME Use (Peyrot and Rubin 2008)

Physicians as Key to Encouraging DSME Use • Educators see physicians as key to encouraging DSME use in patients • Physician recommendations are central factors in patient decisions about health care. • Some physicians (15%) are concerned about losing patients sent to DSME, and 11% of patients report changing physicians as a result of DSME. (Peyrot and Rubin 2008)
")
(Horigan, Davies et al. 2017)
")
(Horigan, Davies et al. 2017)
")
Reasons (Horigan, Davies et al. 2017)
")
Head-to-Head Comparison (Chrvala, Sherr et al. 2016)
")
Cost Savings Associated with Diabetes Education (Duncan, Birkmeyer et al. 2009)

The Real Question is…. . If DSME were a pill, would you prescribe it? (Chrvala, Sherr et al. 2016)
. \"Standards")
Recommendation All people with diabetes should participate in DSME/S. American Diabetes Association (2017). "Standards of medical care in diabetes ".
 Diabetes")
Lifestyle Management 1. 2. 3. 4. 5. 6. 7. Diabetes Self‐management Education (DSME) Diabetes Self‐management Support (DSMS) Medical Nutrition Therapy (MNT) Counseling on Smoking Cessation Education on Physical Activity Guidance on Routine Immunizations Psychosocial Care (American Diabetes Association 2017)

Not every Education have benefits of DSME • Over 10 h in total duration • Follow-up with DSMS • Culturally and age appropriate Culturally age • Tailored to individual needs and preferences • Addressed psychosocial issues and behavioral strategies American Diabetes Association (2017). "Standards of medical care in diabetes ".

Take Home Messages • DSME is the ongoing process & complex activity of facilitating the knowledge, skill, and ability necessary for diabetes self‐care • DSMES is a right for all. • Know 4 critical times to refer for a DSMES Program. • Not every Education have benefits of DSME. • Addressed psychosocial issues and behavioral strategies. • Partnering with diabetes educators to improve patients outcome. • Peer support can help patients on motivations and skills

Thanks for your attention Auguset-2017
- Slides: 58