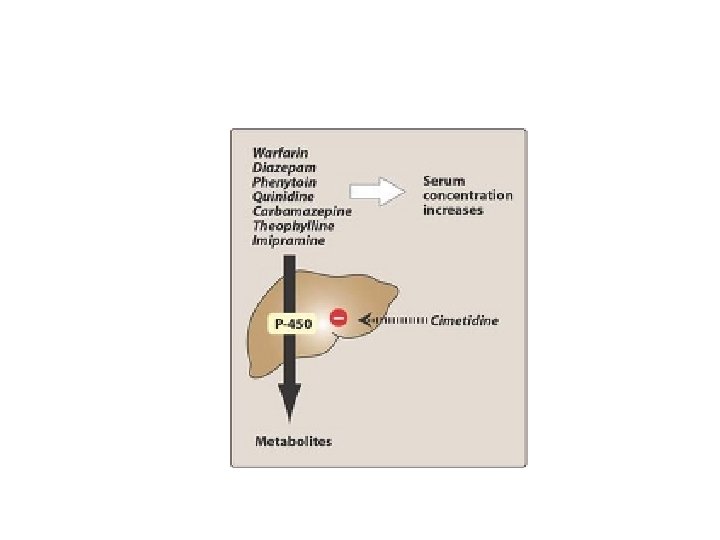
Drugs used to treat GIT disordes Anton Koht











, sucralfate, bismuth subsalicylate • Antibacterial agents")






 • Antacids (containing calcium")

 III. Saline and osmotic laxatives: increase osmotic pressure IV. Stimulant laxatives")



 qthey can damage enterocytes (inflammatory response in the")

 q ACh. E inhibitors (neostigmine) q inhibitory presynaptic D")



 • Antimicrobials (e.")






- Slides: 48
Drugs used to treat GIT disordes Anton Kohút
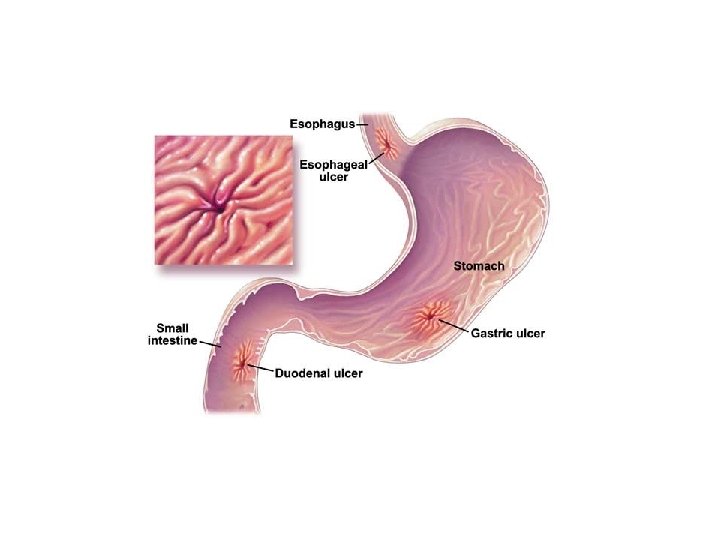
Gastric ulcer
Pathogenesis of Ulcers Therapy is directed at enhancing host defense or eliminating aggressive factors; i. e. , H. pylori. Aggressive Factors l l Acid, pepsin Bile salts Drugs (NSAIDs) H. pylori Defensive Factors l l l Mucus, bicarbonate layer Blood flow, cell renewal Prostaglandins Phospholipid Free radical scavengers
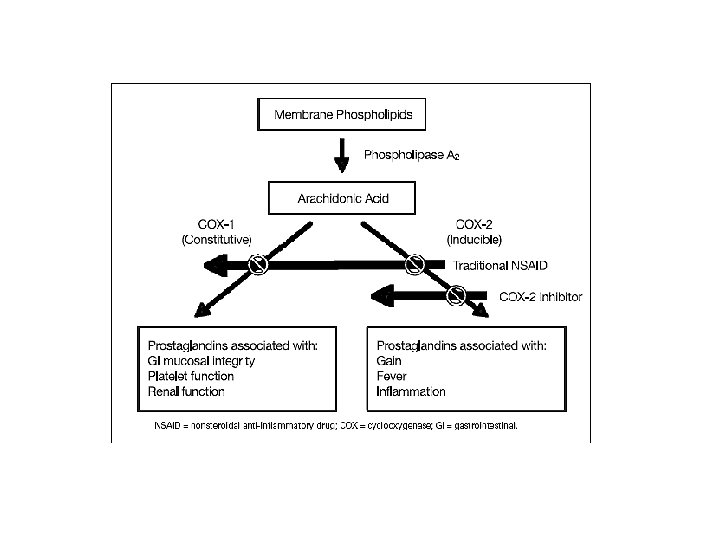
Gastric ulcer and NSAIDs n infection H. pylori
Drugs used to treat gastric ulcer Regulation of gastric acid secretion I. Antisecretory drugs 1. H 2 – blockers: cimetidine, ranitidine, famotidine nisatidine 2. M 1 – blockers: pirenzepine, dicyclomine, propantheline 3. Antagonist of gastrin receptors: somastatine 4. Agonists of PG receptors: misoprostol, entprostyl II. Antacids -sodium bicarbonate, -calcium carbonate, -aluminium hydroxide, -magnesium hydroxide
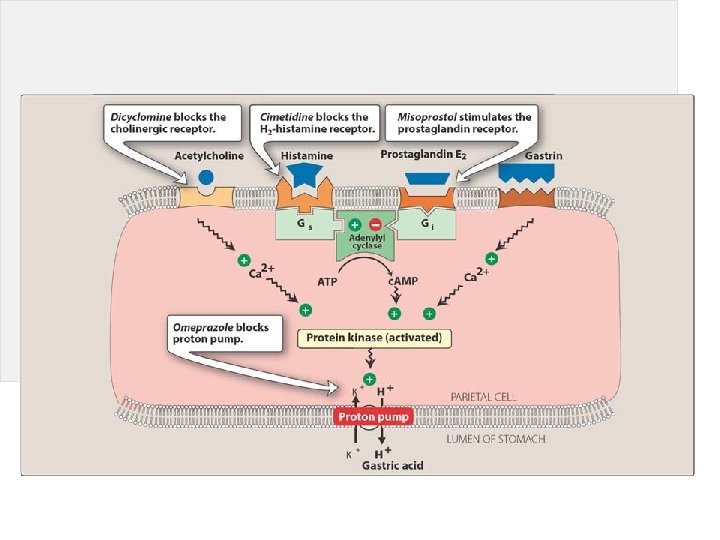
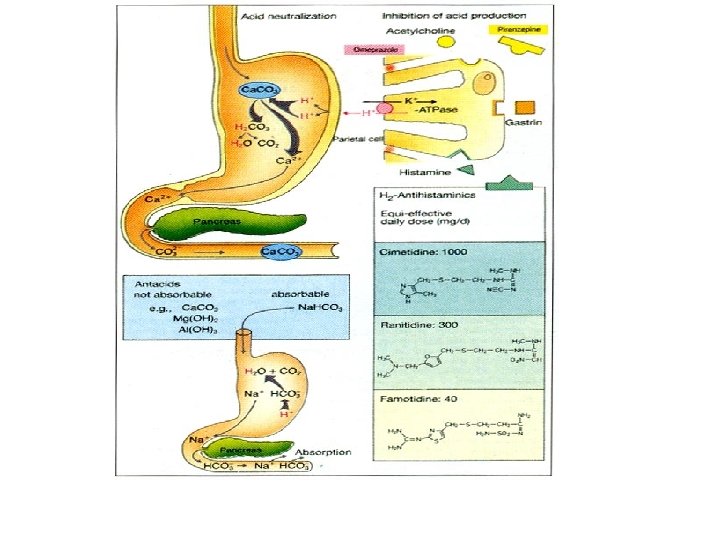
Control of gastric acid secretion
Antisecretory agents 1. H 2 histamine blockers – cimetidine, ranitidine, famotidine, nisatidine 2. Antimuscarinic agents –pirenzepine, dicyclomine, 3. Agonists of prostaglandine receptors misoprostol 4. Antagonist of gastrin receptors- somatostatin 5. Inhibitors of proton pump – omeprazole, pantoprazole
H 2 receptor antagonists
Therapeutic uses of H 2 antagonists n Acute stress ulcers: n in managing acute stress ulcers associated with major physical trauma in high-risk patients in intensive care units. They are usually injected intravenously. n Gastroesophageal reflux disease: Low doses appear to be effective for prevention and treatment of heartburn (gastroesophageal reflux). However, about 50 percent of patients do not find benefit, and PPIs are now used preferentially in the treatment of this disorder. they may not relieve symptoms for at least 45 minutes. Antacids more efficiently, but temporarily, neutralize secreted acid already in the stomach. Finally, tolerance to the effects of H 2 antagonists can be seen within 2 weeks of therapy. n n n
n n n All H 2 antagonists are equally effective in promoting healing of duodenal and gastric ulcers. However, recurrence is common after treatment with H 2 antagonists is stopped (60– 100 percent per year). The use of these agents has decreased with the advent of the PPIs. Patients with NSAID-induced ulcers should be treated with PPIs, because these agents heal and prevent future ulcers better than H 2 antagonists.
Antacids • Calcium containing Calcium carbonate • Magnesium containing Magnesium hydroxide • Aluminium containing Aluminium hydroxide Antacids may decrease absorption of other drugs
• Cytoprotective agents - misoprostol (PGE 1), sucralfate, bismuth subsalicylate • Antibacterial agents colloidal bismuth ATB: ampicilline tetracyclines, metronidazole, clarithromycin
n Sucralfate: - This complex of aluminum hydroxide and sulfated sucrose binds to positively charged groups in proteins of both normal and necrotic mucosa. - By forming complex gels with epithelial cells, sucralfate creates a physical barrier. - Effectively heals duodenal ulcers and is used in long-term maintenance therapy. - Because it requires an acidic p. H for activation, sucralfate should not be administered with H 2 antagonists or antacids.
Bismuth subsalicylate: Effectively heal peptic ulcers. In addition to their antimicrobial actions, They inhibit the activity of pepsin, increase secretion of mucus, and interact with glycoproteins in necrotic mucosal tissue to coat and protect the ulcer crater.
Antibacterial agents Currently, either n triple therapy consisting of a PPI with either metronidazole or amoxicillin plus clarithromycin, n or quadruple therapy of bismuth subsalicylate and metronidazole plus tetracycline plus a PPI, are administered for a 2 -week course. n
GIT motility disorders
GIT motility disorders • Constipation means hard stools, difficulty passing stools, or the sense of incomplete emptying after a bowel movement. • Diarrhoea is a watery stool occurring more than three times in one day. Prolonged diarrhea can be a sign of other problems and it can cause dehydration.
Constipation
Some drugs causing constipation • Analgesics (inhibitors of prostaglandin syntesis) • Antacids (containing calcium carbobate or aluminium hydroxide) • Anticholinergics • Antihistamines (H 1 blockers) • Corticosteroids • Clonidine • Ganglionic blocking agents • Laxatives (used chronically) • Myorelaxants • Opioids • Phenothiazines • Tricyclic antidepresants • Verapamil
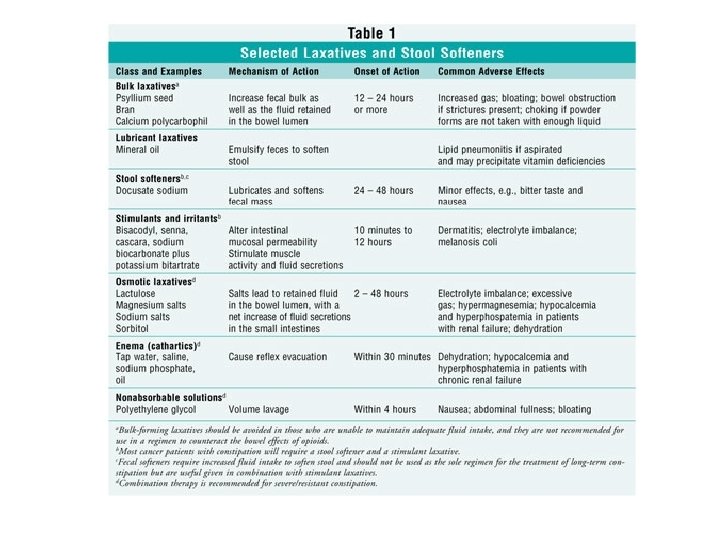
Laxatives I. II. Bulk forming laxatives: high fiber, absorbs water to increase bulk, distends bowel to initiate reflex bowel activity – - polysaccharides and celluloses derived from grains, psyllium, methylcellulose, and carboxymethylcellulose, synthetic resin polycarbophil Emolients- surfactants: stool softeners and lubricants, promote more water and fat in the stools, lubricate the fecal material and intestinal walls -stool softeners: docusate salts, lubricants: mineral oil
Laxatives (cont. ) III. Saline and osmotic laxatives: increase osmotic pressure IV. Stimulant laxatives (contact, iritant) – within the intestinal tract, causing more water to enter the intestines. Result: bowel distention, increased peristalsis, and evacuation magnesium sulfate, magnesium hydroxide, magnesium citrate, sodium phosphate the disaccharide lactulose; glycerin; sorbitol and mannitol; and polyethylene glycol-electrolyte solutions. increases peristalsis via intestinal nerve stimulation : diphenylmethane phenolphthalein, bisacodyl, anthraquinone laxatives, castor oil (ricin, ricinoleic acid) V. Prokinetic agents
Laxatives: Side Effects Bulk-forming laxatives have few side effects and minimal systemic effects: allergic reactions (plant gums) q flatulence q systemic retention of Na+ and H 2 O (psyllium, carboxymethylcellulose) q dextrose should be avoided in diabetic patients q cellulose can reduce the absorption of many drugs (cardiac glycosides, salicylates, nitrofurantoin) q psyllium may bind coumarin derivatives
Saline laxatives q up to 20% of the salt is absorbed q Mg 2+ - toxicity in patients with impaired renal function q Na+ salts should not be used in patients with congestive heart failure or renal disease q phosphate laxatives can cause hyperphosphatemia and a reduction of plasma Ca 2+ q hypertonic salt solutions can produce significant dehydration and must be administered with sufficient water to ensure that no net loss of body water occurs
Hyperosmotic q lactulose: flatulence, cramps, abdominal discomfort q excessive dosage can cause diarrhea, loss of fluid and K+, hypernatremia, exacerbation of hepatic encephalopathy Contraindications q patients requiring a galactose-free diet must not use lactulose q patients with diabetes must be cautious in using lactulose
Stimulants qfluid and electrolyte deficits (overdosage) qthey can damage enterocytes (inflammatory response in the colon) qallergic reactions, osteomalacia qprotein- losing gastroenteropathy qpossible pink coloring of the urine and feces (phenolphthalein) qan excessive laxative effect and abdominal pain (senna, cascara)
Prokinetic agents
q direct M-receptor agonists (bethanechol) q ACh. E inhibitors (neostigmine) q inhibitory presynaptic D 2 -receptor blockers (metoclopramide) q excitatory presynaptic 5 -HT 4 -receptor agonists (cisaprid) q excitatory motilin receptor activators (erythromycin) q prokinetic drugs increase gastric emptying q they increase tone of the lower esophageal sphincter q they exhibit antiemetic activity (metoclopramide) q they improve coordination of gastroduodenal contractions
Side effects q cholinergic agonists have variety of muscarinic side effects (excess GI secretions, cramps, salivation, sweating, urination, lacrimation, defecation) q dopamine-receptor dystonia, antagonists Parkinson´s can induce disease-like effects hyperprolactinemia (gynecomastia, galactorhea
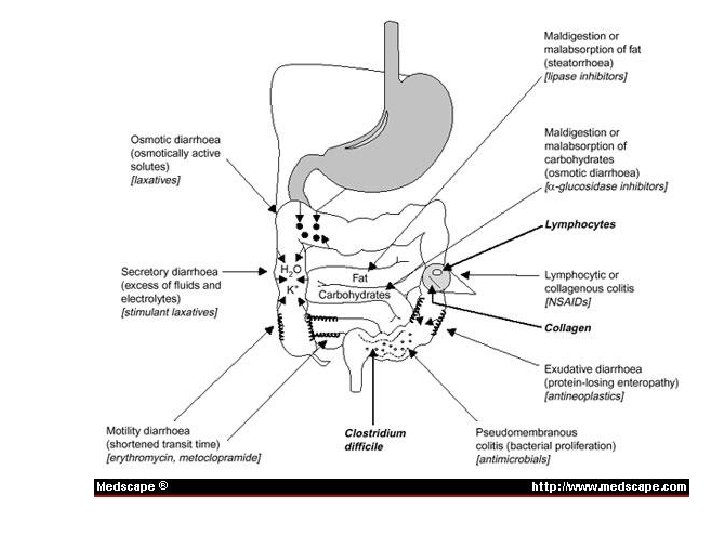
Diarrhoea
Diarrhoea • Traveller’s diarrhoea is one of the most common illnesses for tourists going to tropical climates. As many as 60% of all travellers suffer some form of diarrhoea
Some drugs causing diarrhoea • Adrenergic neuron blocking agents (reserpine, quanethidine) • Antimicrobials (e. g. sulfonamides, tetracyclines, most broad spectrum ATB • Cholinergic agonists and cholinesterase inhibitors • Procinetic agents (metoclopramide, domperidone, cisapride) • Prostaglandins • Quinidine
Antidiarrhoeal drugs I. Opioids: diphenoxylate and loperamide free of opiate – like CNS effect, opium tincture, codeine, decrease bowel motility, decrease transit time through the bowel, allowing more time for water and electrolytes to be absorbed, opioids are effective in the treatment of moderate-to-severe diarrhea! III. Octreotide (the synthetic analog of somatostatin) inhibition of gastric acid and pepsinogen secretion, inhibition of endocrine secretions (e. g. , gastrin, cholecystokinin, secretin, VIP, and motilin), inhibition of intestinal fluid and bicarbonate secretion, and diminution of smooth muscle contractility.
IV. Other Agents a. Adsorbents: kaolin, pectin, bismuth subsalicylate, activated charcoal coat the walls of the GI tract, bind to the causative bacteria or toxin, which is then eliminated through the stool b. Intestinal flora modifiers : lactobacili (supplying missing bacteria to the GI tract, suppressing the growth of diarrhea-causing bacteria), c. Muscarinic antagonists b. fiber supplements - adsorbents (psyllium, polycarbophil, carboxymethylcellulose) - increase the viscosity of feces
Antiemetics
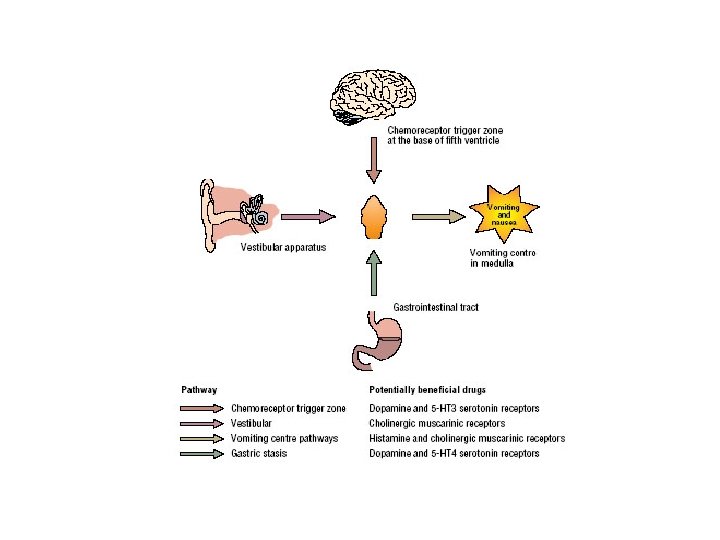
Receptors involved in vomiting
Causes of vomiting I. Drugs • Anticancer drugs, cardiac glycosides, apomorphine, levodopa, bromocryptine, cholinomimetics, opiates, ergot alkaloids II. Physiological • Pregnancy, head motion, weitghlesness III. Pathophysiological • Uremia, endocrinopathies, alcoholism, migraine, allergies, • gastric irritations IV. Toxic • Food poisons, industrial poisons, radiations, infections
Recomended antiemetic treatment