Principles of pharmacodynamics Anton Koht How drugs act

 act")





 l Affinity - tendency to bind to the receptors (attraction")

 non-competitive antagonism a. form bonds with the receptors usually at")

 Receptor ( 1 -2)")





 Percentage of maximum effec Semilogaritmic - effect of the")
 efficacy slope of the curve 50% EC 50 10")




 and tolerance The loss of a drug’s effect, commonly seen when it")

 over a short")
 E")



- Slides: 44
Principles of pharmacodynamics Anton Kohút
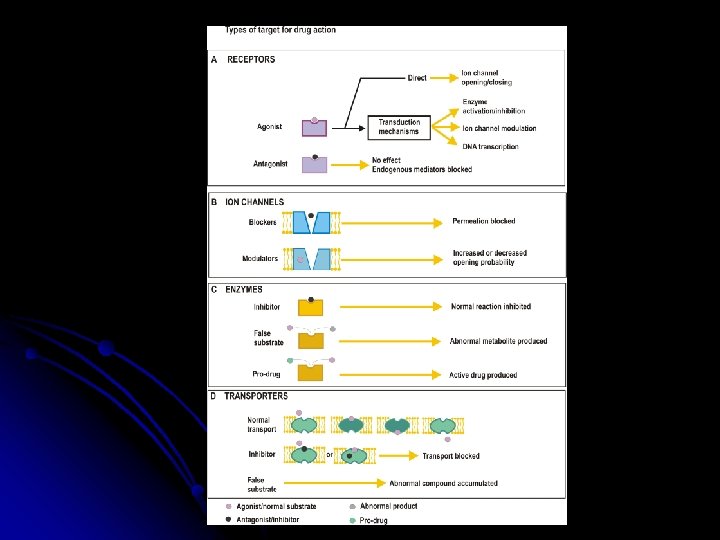
How drugs act? l Indirectly only a few drug (osmotic diuretics, general anesthetics) act on the base their physicochemical properties they need no specific binding site l Directly drugs interact with specific protein macromolecule special regulatory proteins: 1. enzymes 2. ion channels 3. carrier molecules 4. receptors
Targets - regulatory proteins 1. 2. . Receptors Enzymes aspirin COX neostigmine ACh. E methotrexate DH-folate reductase digoxin Na+-K+-ase allopurinol xanthine oxidase omeprazole H+/K+- ATPase 3. Ion channels Ca, Na, K 4. Carrier molecules transport of glucose, amino acids transport in renal tubules re-uptake of neurotransmiters (NA, 5 -HT)
No drugs are completely specific in their actions. In many cases, increasing the dose of a drug will cause it to affect targets other than the principal one, and this can lead to sideeffects. l
Receptors
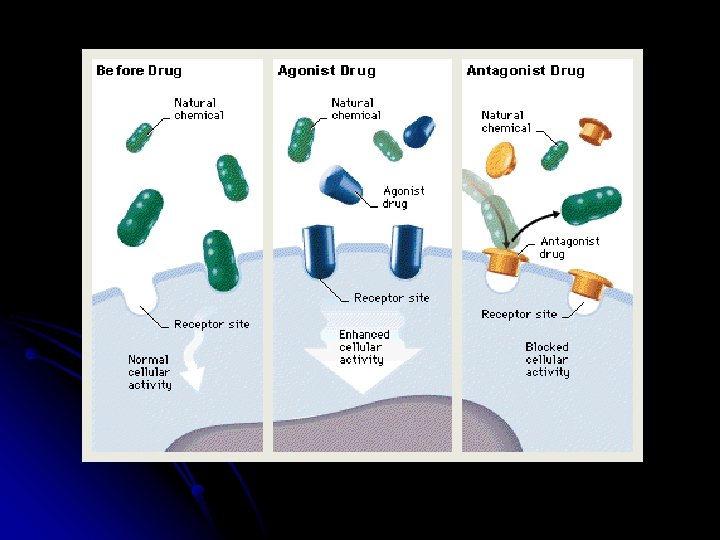
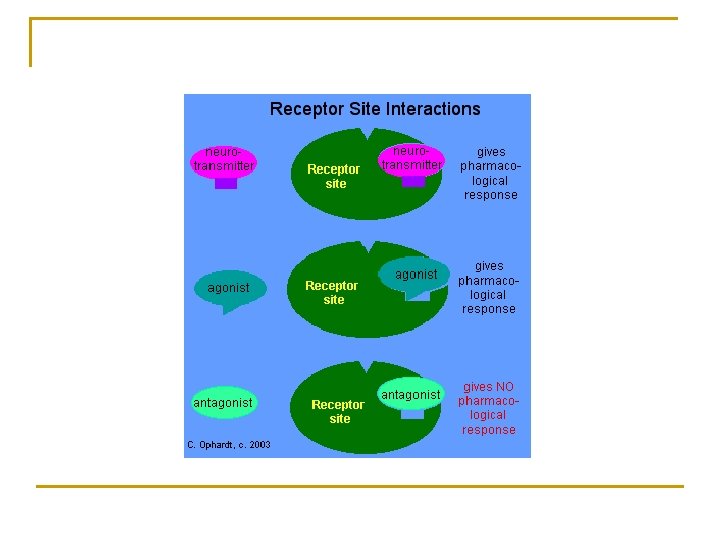
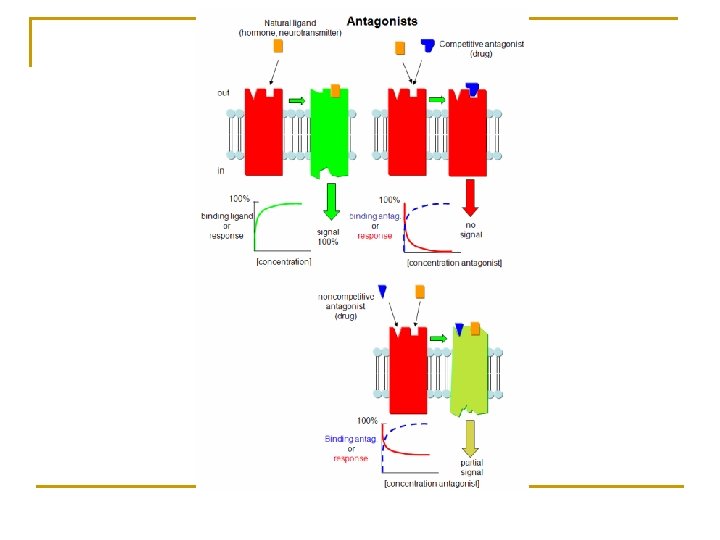
Regulatory proteins – receptors drugs act on receptors as agonists or antagonists 1. Agonists bind to receptors and produce a responseeffects of various types 2. Antagonists bind to receptors without producing a response and by occupying the receptors they prevent action of agonists.
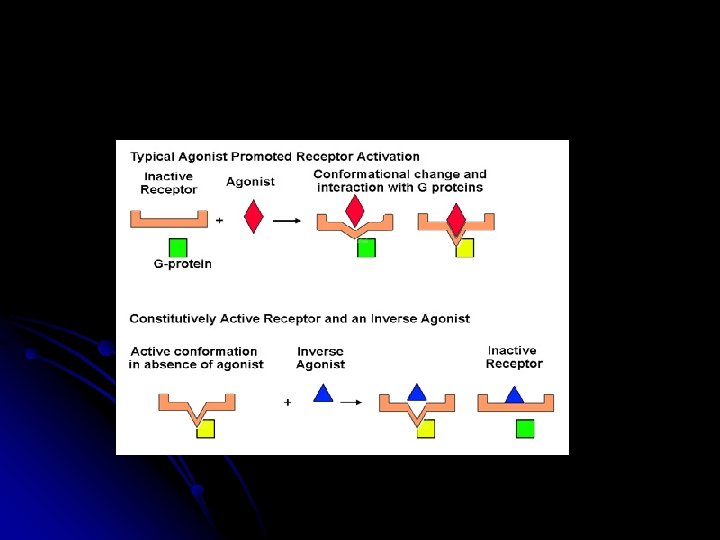
1. Agonists agonist I - the drug binds to the same site as the endogenous compounds and produce the same type of action agonist II - the drug binds to a different site than does agonist I - allosteric action inverse agonist – produces inactivation of active receptor
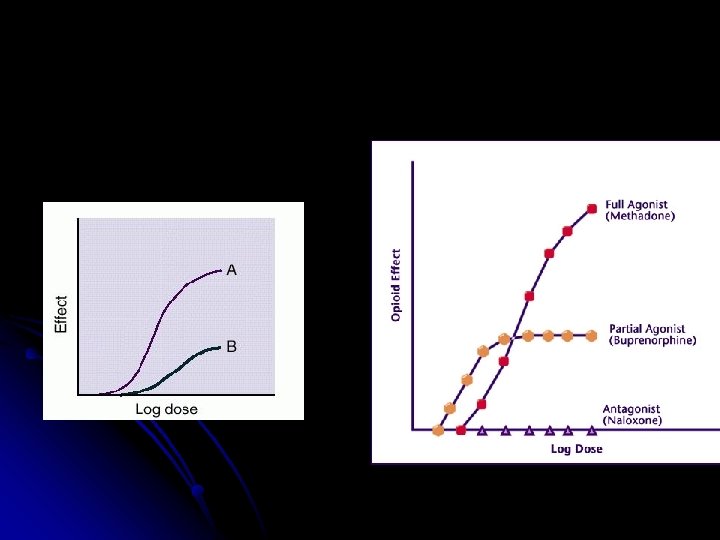
1. Agonists (cont. ) l Affinity - tendency to bind to the receptors (attraction between receptor and drug) l Efficacy - ability once bound, to initiate changes, which lead to effect (is the capacity of drug to activate a receptor) Full agonists - can produce maximal effect when all receptors are occupied (high efficacy) Partial agonists - can produce only submaximal effects even when all receptors are occupied
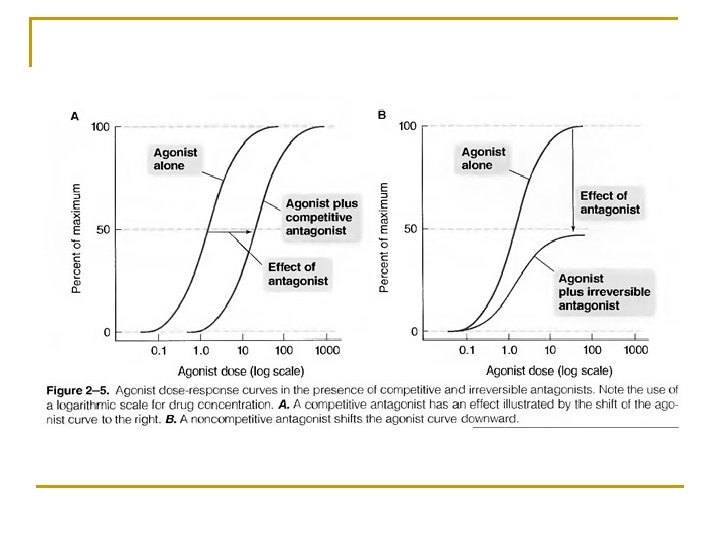
2. Antagonists l competitive antagonism antagonists are able to displace the agonists from the receptors (one drug can be displaced by another drug), may be abolished by adding an excess of agonist. a. reversible b. ireversible antagonist dissociates very slowly or not
2. Antagonists (cont. ) non-competitive antagonism a. form bonds with the receptors usually at sites other than the endogenous agent. b. in some cases binding may be covalent and ireversible c. cannot be overcom by higher concentration of agonist
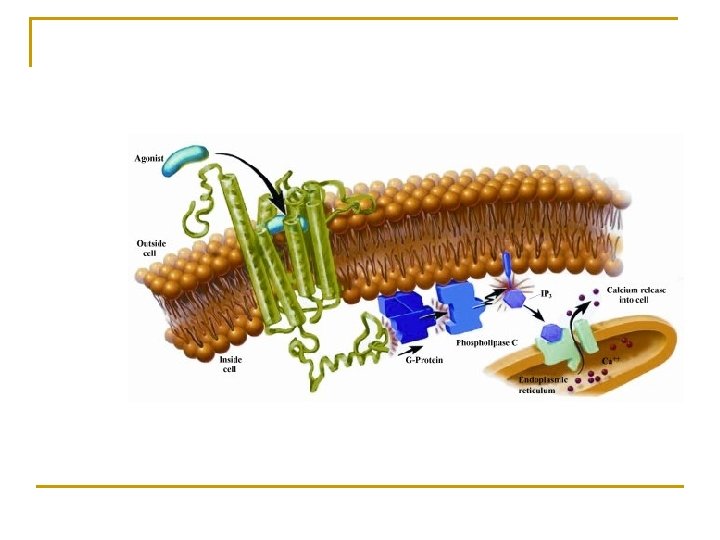
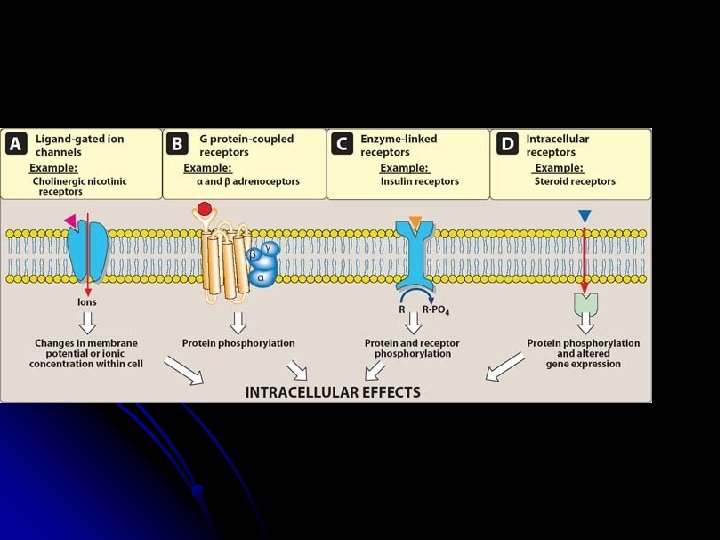
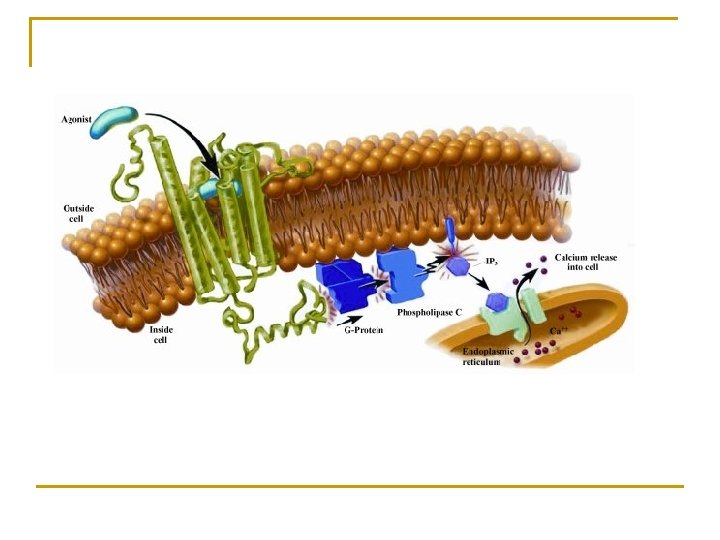
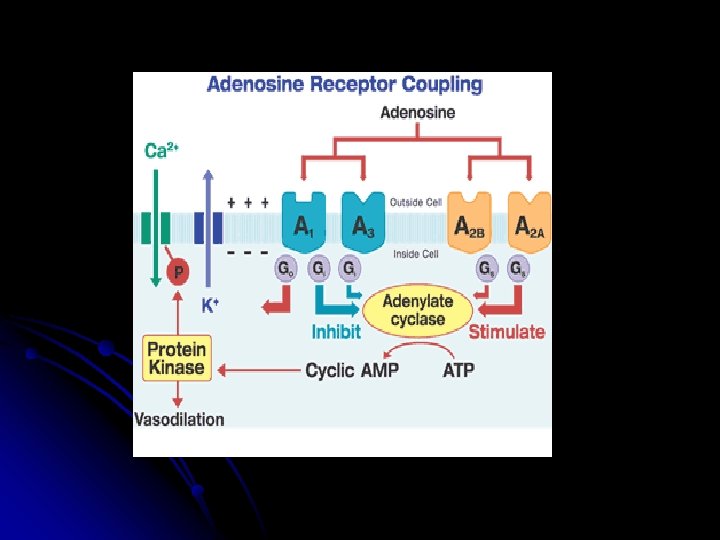
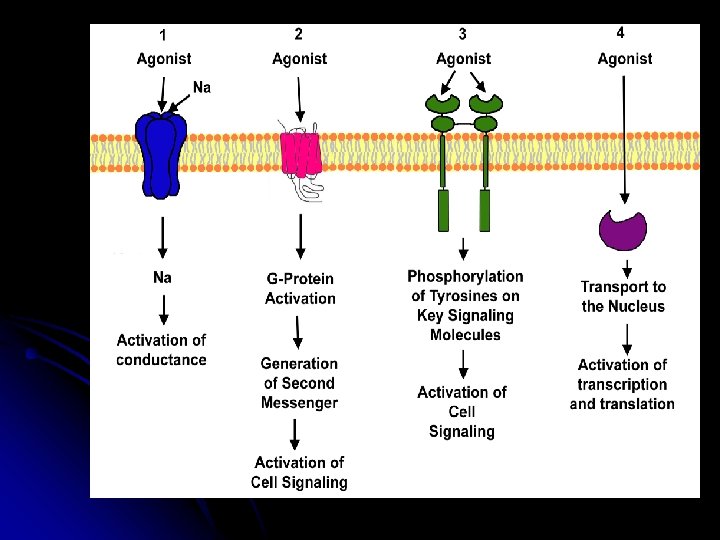
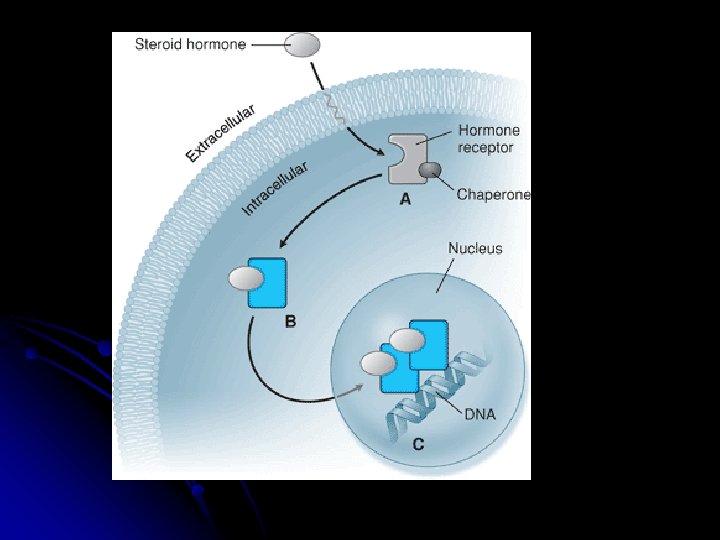
Receptors –types of receptors A. for fast neurotransmitters - coupled directly to an ion channel, e. g the nicotinic ACh receptor, GABA, glutamate, 5 -HT 3 B. coupled to G-protein - for many hormones and slow transmitters (neurohormonal receptors), muscarinic ACh receptors, adrenergic receptors C. coupled to tyrosine kinase - for insulin and various growth factors, D. cytosolic receptors - for steroids (are usually slow)
Adrenergic beta receptor Transduction system l l l Agonist (noradrenaline) Receptor ( 1 -2) G-protein (Gs, Gi) Effector enzyme (adenylcyclase, AC) Second messenger (c. AMP) Drug action
Adrenergic beta receptor
Cholinergic receptor
Receptors - localization
Mechanism of action of intracellular receptors A lipid-soluble drug diffuses across cell membrane and moves to the nucleus of the cell Drug TARGET CELL CYTOSOL Drug Inactive receptor NUCLEUS The drug binds to an intracellular receptor. Activated receptor complex Gene m. RNA The drug-receptor complex binds to chromatin, activating the transcription of specific m. RNA genes. Specific proteins according to Lippincott´s Pharmacology, 2006) Biologic effects
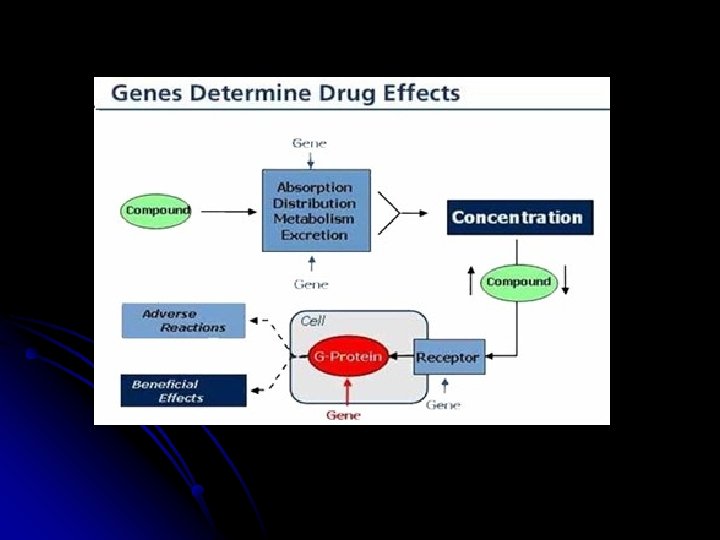
DOSE-RESPONSE RELATIONSHIPS A agent that can bind to a receptor and elicit a response. magnitude of the drug effect depends on its concentration at the receptor site, which in turn is determined by the dose of drug and by factors characteristic of the drug (e. g. rate of absorption, distribution, metabolism).
(according to Lippincott´s Pharmacology, 2006) Percentage of maximum effec Semilogaritmic - effect of the dose on the magnitude of pharmacologic response. 100 Drug A Drug B 50 EC 50 0 log [Drug] The potency of drug can be compared using the EC 50, the smaller the EC 50 the more potent the drug.
effect Log-concentration-effect curve potency (affinity) efficacy slope of the curve 50% EC 50 10 -8 10 -7 10 -6 10 -5 10 -4 c
Drug A is more potent than Drug B, but both show the same efficacy. Biologic effect Typical doseresponse curve for drug showing differences in potency and efficacy. (EC 50 = drug dose that shows fifty percent of maximal response. ) Drug C shows lower potency and lower efficacy than Drugs A and B. 100 50 Drug A Drug B Drug C 0 Log drug concentration (according to Lippincott´s Pharmacology, 2006) EC 50 for Drug A EC 50 for Drug B Drug C
3. Antagonism by receptor block Antagonists in this sense are the drugs that bind to receptors activate them. a) Reversible competitive antagonism: b) competitive antagonists bind reversibly with receptors at th c) as the agonist. The response can be returned to normal by increasing the dos ! Competitive antagonist has no intrinsic efficacy ! Reversible competitive antagonism is the commonest and mo important type of antagonism; Two main characteristics: ― in the presence of the antagonist, the agonist log DRC is sh the right without change in slope or maximum, the extent of being a measure of the dose ratio ― the dose ratio increases linearly with antagonist concentrat
Biologic effect Effects of drug antagonists Drug alone Drug with non- Drug with competitive antagonist Drug concentration EC 50 or drug alone or in (according to Lippincott´s presence of a Pharmacology, 2006) noncompetitive EC 50 for drug in the presence of a competitive
Variation in receptor numbers Continued stimulation or inhibition of living systems tends to induce compensatory processes. Thus individuals continually exposed to an agonist predictably require larger doses to achieve a given effect than would a naive subject. This tolerance is thought to results from a decrease in reception numbers - down- regulation. ( The opposite may also occur: in patients on long-term beta-blocker therapy, it is thought that catecholamine receptor numbers are increased - up-regulation the tendency to a marked rise in blood pressure if the drug is stopped suddendly (rebound hypertension).
Desensitisation (tachyphylaxis) and tolerance The loss of a drug’s effect, commonly seen when it is given repeatedly or continuously. Ø The onset and recovery : Øvaries from seconds to minutes (called TACHYPHYLAXIS) Ø to days or weeks (called TOLERANCE) Many mechanisms: ― changes in receptors ― loss of receptors (down regulation) ― exhaustion of mediators ― enhanced drug metabolism ― active efflux of drugs ― compensatory physiological mechanisms
Desensitization of receptors - -- down-regulation - types of desensitization - when receptors are (they undergoe endocytosis – they are not available for further agonist action). These receptors may be recycled to the cell surface, restoring sensitivity, or may be further degraded, decreasing the total number of receptors available. Some receptors (particularly voltage-gated channels) - they require a rest period following stimulation before they can be activated again. During this recovery phase they are said to be "refractory" or "unresponsive. "
Desensitization of receptors Repeated administration of an agonist (such as epinephrine) over a short time period, results in diminished response of the cell. Response tachyphylaxis Time 0 0 0 50 10 40 20 30 30 30 Repeated injection of drug (according to Lippincott´s Pharmacology, 2006) Following a period of rest, administration of the drug results in a response of the original
Tachyphylaxis after repeated administration of ephedrine (decrease in its effect on blood pressure) E = administration of ephedrine
Percentage of patients Cumulative percentage of patients responding to plasma levels of a drug B: Penicillin: Large therapeutic index Therapeutic window 100 50 0 Desired therapeutic effect Unwanted adverse effect Log concentration of drug in plasma (arbitrary units) (according to Lippincott´s Pharmacology, 2006)
QUANTAL DOSE-RESPONSE CURVES LD 50 TI = ----ED 50 Therapeutic range = TD 50 - ED 50
Therapeutic index The ratio of the dose that produces toxicity to the dose that produces a clinically desired or effective response in a population of individuals: Therapeutic index = LD 50/ED 50 or TD 50/ED 50 TD 50 = the dose that produces a toxic effect in half the population, LD 50 = the dose that produces a death in half the population ED 50 = the dose that produces a therapeutic or desired response in half the population. The therapeutic index = a measure of a drug's safety – a large value = there is a wide margin between doses that are effective and toxic.