GIT Bleeding Acute Upper GIT Hemorrhage Lower GIT


GIT Bleeding Acute Upper GIT Hemorrhage Lower GIT Bleeding Occult GIT Bleeding

This is the most common GIT emergency Accounting for 50 -120 admissions to hospital per 100 000 of the population each year in the United Kingdom.
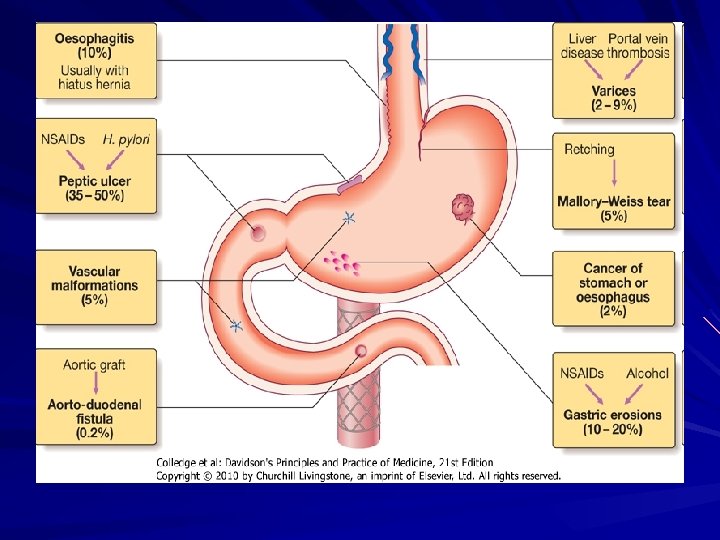

Diagnosis % Comments Peptic ulcer 35 -50% Dyspepsia or history of peptic ulcer Bleeding may be precipitated with NSAIDs or alcohol Gastric 10 -20% Associated with NSAIDs & erosions Alcohol Esophagitis 10% Heartburn not invariable & bleeding usually not severe Mallory 5% Follows vomiting or retching Weis tear e. g. after alcohol binge

Diagnosis % Vascular 5% malformations Comments Varices Usually with evidence of liver disease Chronic blood loss usually present 2 -4% Carcinoma 2% (esophagus or stomach) Aorto-enteric 1% fistula Associated with aortic valve disease or hereditary hemorrhagic telangiectasia Consider in any patient who presents after aortic graft surgery

Hematemesis may be: – Red with clots when bleeding is profuse OR – Black “Coffee ground” when bleeding is less severe. Syncope Symptoms of anemia (chronic bleeding). Melaena is the term used to describe the passage of black, tarry stools containing altered blood. It is due to: – Bleeding from the upper GIT (usually) – Hemorrhage from the right side of the colon (occasionally) Hematochezia (maroon or bright red stool) may be found sometimes in cases of severe acute upper GIT bleeding.

Monitoring Intravenous access Initial clinical assessment Endoscopy Acute upper GIT Bleeding Blood Tests Oxygen Resuscitation

The first step is to gain intravenous access using at least one large bore canula.

Define circulatory status: – Severe bleeding causes tachycardia, with hypotension and oliguria – The patient is cold, sweating and may be agitated. Seek evidence of liver disease: – – Jaundice Cutaneous stigmata Hepatomegaly Ascites Define comorbidity (cardio-respiratory, cerebrovascular & renal): – They might be worsened by upper GIT bleeding – They increase the hazards of Endoscopy & surgical operations.

Full Blood Count: – Chronic or Subacute bleeding may cause anemia – Hb concentration might be normal in cases of sudden , major bleeding until hemodilution occurs. Urea & electrolytes. Liver function tests Prothrombin time: (if there is clinical suggestion of liver disease or in anticoagulated patients) Cross matching of at least 2 units of blood.

IV crystalloid or colloid: – They are given to restore blood volume: Blood transfusion if: – The patient is shocked – Hb concentration < 10 gm/dl. Normal saline must be avoided in patients with liver disease Central Venous Pressure (CVP) monitoring (severe bleeding, patients with heart disease) – It help to define the volume of fluid replacement – It help in identification of rebleeding.

This should be given by facemask to all patients in shock

Should be carried out after adequate resuscitation Can reach diagnosis in 80% of cases Can be used in treatment of patients with major endoscopic stigmata of recent hemorrhage including: – Active spurting hemorrhage – Visible vessel (pseudo-aneurysm) Endoscopic treatment modalities include: – Thermal modality e. g. heater probe – Injection of dilute adrenalin into the bleeding point – Application of metallic clips

Endoscopic therapy are useful for: – Stopping active bleeding – Preventing rebleeding – Avoiding the need for surgery Endoscopic therapy is also used for: – Varices – Vascular malformations – Mallory-Weiss tears.

If endoscopy is normal despite active bleeding: – Radiolabelled red cell scanning or visceral angiography (if the patient is actively bleeding by at least 1 ml/minute) – Colonoscopy (for bleeding of lesser severity) – the most common cause is vascular malformations – 99 Tc-pertechnate scan may show bleeding from Meckel’s diverticulum. Wireless cap. prior to enterosc. • Patients are closely observed with hourly: • Pulse rate • Blood pressure • Urine output

An urgent surgical operation is undertaken when: – Endoscopic hemostasis fails to stop active bleeding – Rebleeding occurs on: One occasion in an elderly or frail patient Twice in younger, fitter patients.

ACUTE UPPER GIT HEMORRHAGE role of endoscopic therapy Meta-analysis of 21 RCTs shows that endoscopic therapy (injection of adrenalin into the bleeding point, application of thermal energy or electrocoagulation) reduces: – Ulcer rebleeding rate – The need for urgent surgery – Hospital mortality rates.

Bleeding Ulcers adjunctive drug therapy “intravenous proton pump inhibitor” infusions, when given to patients who have been subjected to endoscopic therapy for major peptic ulcer hemorrhage, reduce: – Rebleeding rate – Need for surgery – BUT NOT mortality

Mortality after admission to hospital is approximately 10%

Risk factors for death in patients who present with acute upper GIT bleeding Factor Increasing age Comments Risk increases over age 60 & especially in very elderly Comorbidity Advanced malignancy, renal & hepatic failure associated with particularly high mortality Shock Defined as: pulse > 100/min, BP < 100 mm Hg

Risk factors for death in patients who present with acute upper GIT bleeding Factor Diagnosis Comments Varices & cancer have the worst prognosis Endoscopic Active bleeding & non-bleeding findings visible vessel at Endoscopy are associated with a high risk of continuing bleeding Rebleeding* Associated with 10 folds rise in mortality *defined as fresh hematemesis or melena associated with shock or fall of Hb > 2 gm/dl over 24 hours


It may be due to hemorrhage from: – Small bowel – Colon – Anal canal You must distinguish between: – Profuse acute bleeding – Chronic or subacute bleeding

Severe acute: – – Diverticular disease Angiodysplasia Ischemia Meckel’s diverticulum Moderate, chronic/subacute: – Anal disease e. g. fissure, hemorrhoids – Inflammatory bowel disease – Carcinoma – Large poylps – Angiodyplasia – Radiation enteritis – Solitary rectal ulcer

This is an unusual medical emergency Patients present with profuse red or maroon diarrhea and with shock Diverticular disease: – It is the most common cause – Acute bleeding is due to erosion of an artery within the mouth of a diverticulum – Bleeding almost always stops spontaneously.

Angiodysplasia: – It is disease of elderly, in which vascular malformations develop in the proximal colon – It is most commonly seen in patients receiving anticoagulants following aortic valve replacement. – Can be acute and profuse bleeding – It usually stops spontaneously but usually recurs. – Diagnosis: Colonoscopy: vascular spots (reminiscent of spider naevi) Visceral angiography: Bleeding into the intestinal lumen & an abnormal large draining vein Laparotomy with on-table colonoscopy – Treatment: Endoscopic thermal ablation Right hemicolectomy (sometimes necessary in severe cases).

Ischemia: – It is due t occlusion of the inferior mesentric artery – It presents with abdominal colic and rectal bleeding – It should be considered in patients (particularly the elderly) who have evidence of generalized atherosclerosis.

Meckel’s diverticulum: – Meckel’s diverticulum with ectopic gastric epithelium may ulcerate and erode into a major artery. – The diagnosis should be considered in children or adolescent present with profuse or recurrent lower GIT bleeding – Meckel’s scan is sometimes positive – The diagnosis is commonly made by laparotomy only at which time the diverticulum is excised

It is extremely common at all ages It is usually due to hemorrhoids or anal fissures Hemorrhoidal bleeding is: – – Bright red Occurs during or after defecation Proctoscopy is used to reach diagnosis Colonoscopy or barium enema is necessary to exclude coexisting colorectal carcinoma, is indicated in: Patients who also have altered bowel habits All patients presenting over 40 years of age. Anal fissure should be suspected when fresh rectal bleeding and anal pain occur during defecation

Occult means that blood or its breakdown products are present in the stool but can not be seen It may reach 200 ml/day It causes iron deficiency anemia It signifies serious GIT disease The most important cause is colorectal carcinoma Diagnosis initially by fecal occult blood (FOB) test

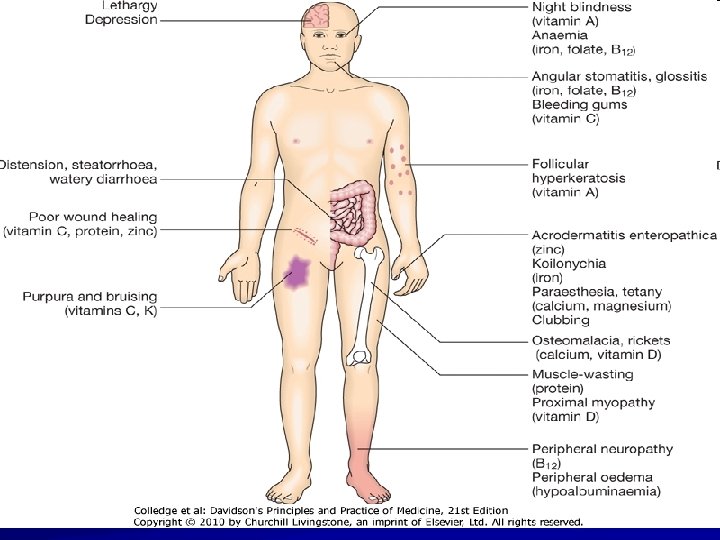
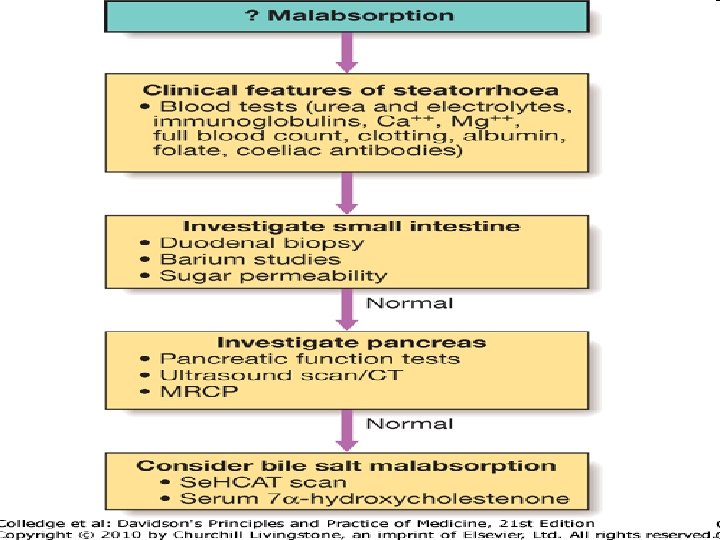
DIARRHOEA Acute Diarrhea < 10 d infective , drugs ( antibio. , NSAID, PPI, Cytotoxic ) Chronic or Relapsing Diarrhea Colonic Small Bowel Malabsorption Clinical feature , causes , investigation


Gastro Esophageal Reflux Disease GERD

GERD resulting in heartburn affects approximately 30% of the general population

Abnormal lower Esophageal Sphincter • Reduced tone • Abnormal relaxation Delayed gastric Emptying Hiatus Hernia Increased intra-abdominal pressure Defective Esophageal Clearance Reflux of acid pepsin (bile) Dietary Factors Gastroesophageal reflux

Abnormalities of Lower Esophageal sphincter reduced lower esophageal sphincter tone inappropriate sphincter relaxation

Hiatus Hernia Occurs in 30% of the population over the age of 50 years Often asymptomatic Heartburn & regurgitation may occur Gastric volvulus may complicate large para-esophageal hernias It causes GERD because: – The pressure gradient between the abdominal & thoracic cavities is lost – The oblique angle between the cardia and esophagus disappears Almost all patients who develop esophagitis, Barret’s esophagus or peptic strictures have hiatus hernia

Delayed esophageal clearance Defective esophageal peristaltic activity It is a primary abnormality Poor esophageal clearance leads to increased acid exposure time

Gastric Contents – Gastric acid is the most important esophageal irritant – There is close relationship between acid exposure time & symptoms Defective gastric emptying

Dietary & environmental factors Material that cause relaxation of the lower esophageal sphincter: – Dietary fat – Chocolate – Alcohol – Coffee There is little evidence to incriminate smoking or NSAIDs as causes of GERD

Clinical features Heartburn & Regurgitation: – Often provoked by: Bending Straining Lying down Waterbrash (Salivation due to reflex salivary gland stimulation as acid enter the gullet) History of weight gain Chocking due to laryngeal irritation by refluxed fluid Odynophagia & dysphagia Atypical chest pain which: – – – Might be severe Might mimic anginal chest pain Is due to reflux induced esophageal spasm.
- Slides: 45