Diagnosing Chronic Venous Insufficiency Khusrow Niazi MD FACC















 to elicit reflux")





- Slides: 25
Diagnosing Chronic Venous Insufficiency Khusrow Niazi, MD, FACC, FSCAI Director Peripheral Vascular Interventions Emory University Atlanta, Georgia
Disclosures: Khusrow Niazi, MD Research Grants: Trireme Surmodics Medtronic Phillips
How many of us have our patients take off their shoes/socks?
Annual Incidence and Prevalence Venous reflux disease is 2 x more prevalent than coronary heart disease (CHD) and 5 x more prevalent than peripheral arterial disease (PAD)1 Venous Reflux Disease Coronary Heart Disease Peripheral Arterial Disease Congestive Heart Failure Stroke Cardiac Arrhythmias Heart Valve Disease -5 5 15 25
Risk factors - Heredity - Age - Female sex - Obesity - Pregnancy - Prolonged standing - Greater height
SPECTRUM OF VARICOSE VEINS • Leg Pain or Aching or Heaviness • Leg Cramps or Tingling • Leg Swelling or feeling of swelling • Itching • Restless Legs • Varicose veins • Spider Veins • Blood Clots • Bleeding • Ulcers
Location of Ulcer J Vasc Surg 2007; 45: S 5 -S 67
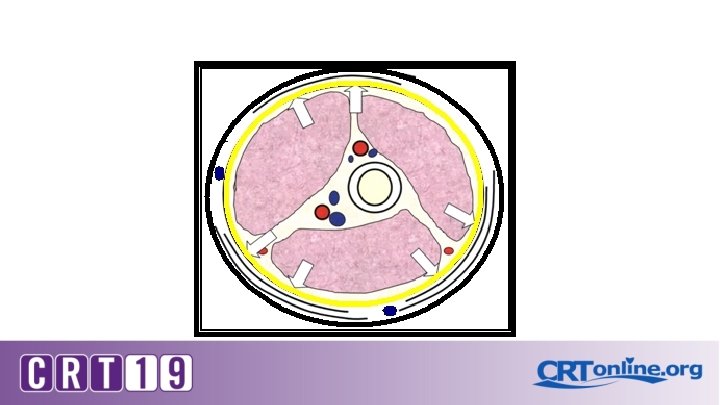
External Iliac v. Common Femoral v. Deep Femoral v. Popliteal v. Gastrocnemius vv. Soleal v. Post Tibial vv
Femoral v. Ant accessory great saphenous v. Great saphenous v. Post accessory great saphenous v.
Intersaphenous v. Cranial extension of the small saphenous v. Popliteal v. Small saphenous v. Dorsal venous arch
Reflux via incompetent valves Venous HTN Venous outflow obstruction Failure of calfmuscle pump
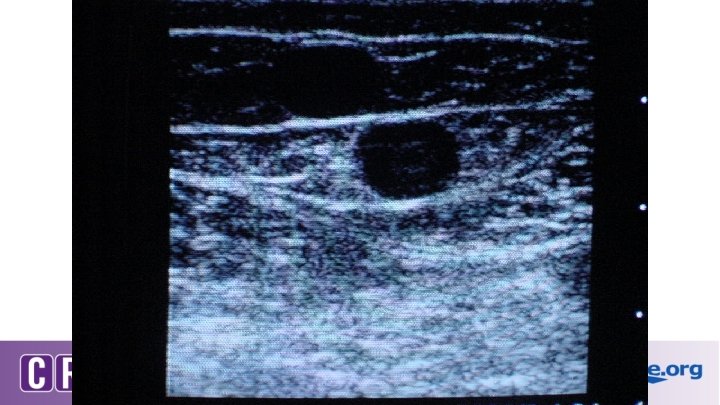
Ultrasound Diagnostic Study � Required in order to determine the source of reflux � Evaluate for venous occlusion or thrombus � Map the course of the incompetent superficial veins
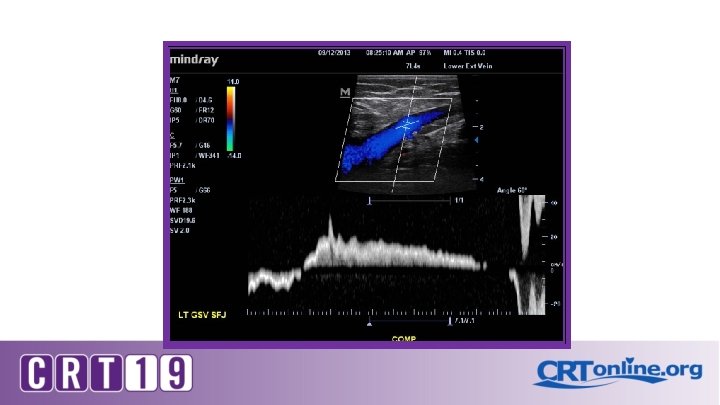
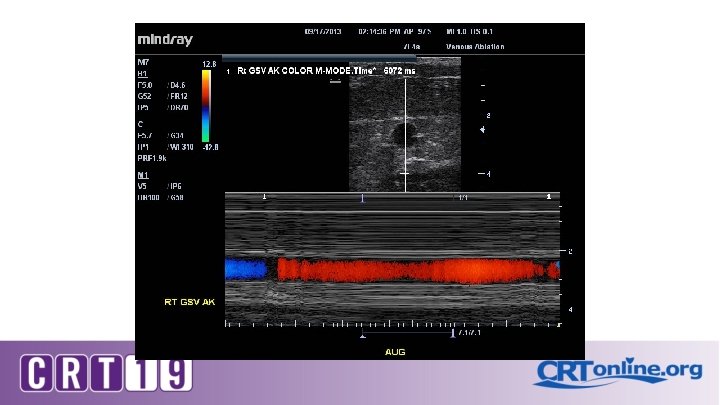
Patient position Erect, semi-erect or reverse Trendelenburg Proximal compression (or Valsalva) to elicit reflux for thigh veins Calf compression of distal veins Flow reversal duration
On Ultrasound: Grey scale , color and Doppler Compressibility Phasic flow Augmentation Perforators Reflux and its duration Vein diameters
Diagnostic testing for Venous insufficiency CVI Venous Doppler *technique* S. V. reflux >3 secs Stasis ulcer Stasis dermatitis S. V. reflux >3 secs Deep vein reflux No reflux Vein diameter Symptoms Compression stockings Ablation