VENOUS ULCERS Venous ulcers Chronic skin and subcutaneous

VENOUS ULCERS

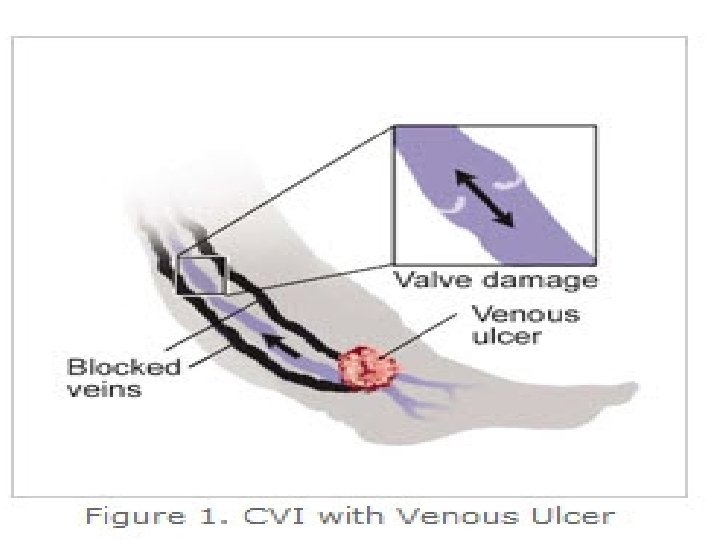
Venous ulcers • Chronic skin and subcutaneous lesions • Venous ulcers are wounds that are thought to occur due to improper functioning of venous valves, usually of the legs (hence leg ulcers )

Venous ulcers • Found on the lower extremity at the pretibial and the medial supra-malleolar areas of the ankle • known as “venous stasis” ulcers because their development was thought to be caused by blood pooled in the veins.

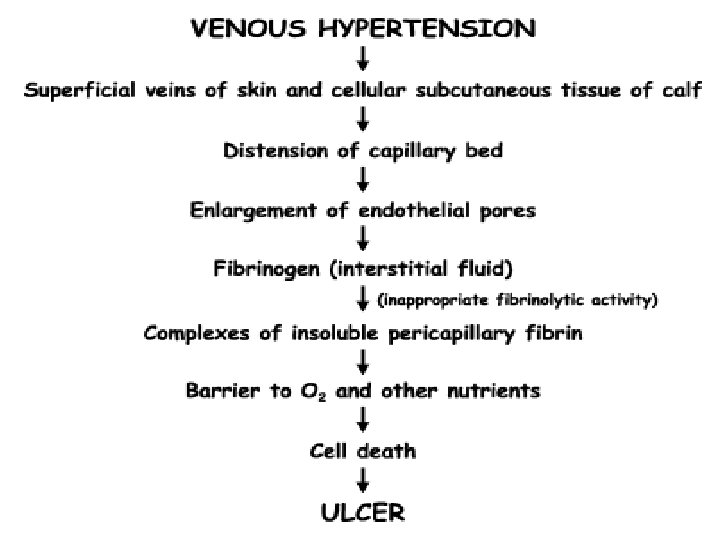
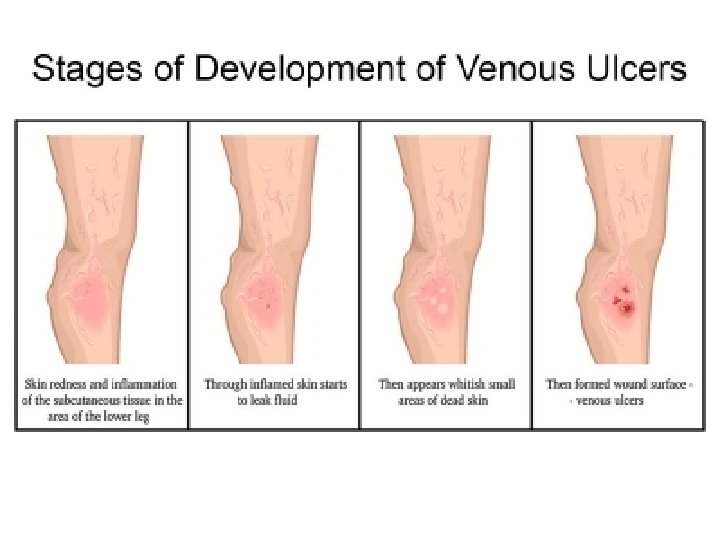
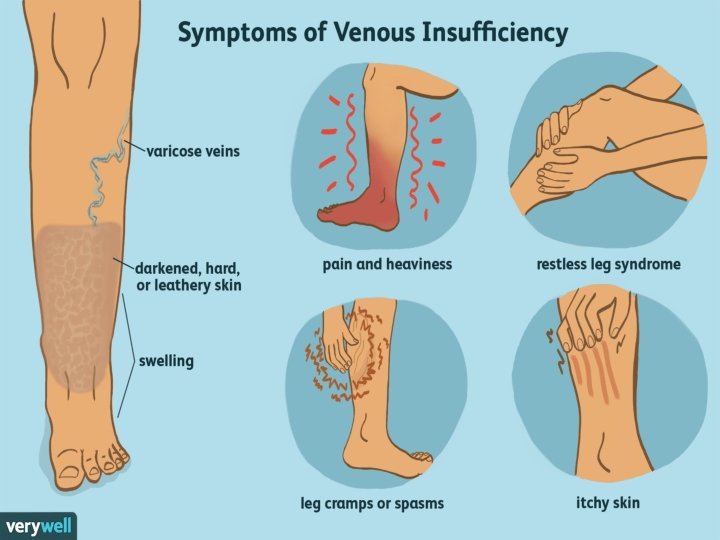
CHARACTERISTICS OF VENOUS ULCERS • Venous hypertension- edema of venous insufficiency. • Leakage of red blood cells occurs through these compromised veins. • “internal tattooing” of the skin- Hemosiderin deposit. • Skin shiny and subsequently sclerotic, giving a taut skin appearance in these areas • Edema and loss of red cells into the subcutaneous tissue occur at the point of greatest gravitational pressure, the ankle.

• venous stasis, hyper pigmentation of the subcutaneous tissues. • the characteristics of long-standing venous insufficiency called lipodermatosclerosis • Many patients with venous insufficiency—even those in whom the condition is mild—report nocturnal leg cramps. • fluid distention of the muscular cells, causing tetanic-like contractions of various muscle groups. • The appearance of telangiectasias, more commonly called “spider veins, ” is the result of distention of the smaller subdermal capillary network. • Venous aneurysms due to massive dilation of the greater saphenous vein and its tributaries.

• stagnation of flow thrombophlebitis Thrombosis adheres to the wall of the vein valves remain incompetent to compensate for the reduced venous return, the surrounding collateral veins dilate Increased venous pressure impedes capillary flow, decreasing oxygen available Tissue damage, scar formation and, ultimately, ulceration. • In varicose veins, the endothelial-enhanced noradrenaline vasoconstriction is decreased. • Endothelial damage is thought to be a possible cause of venous dilatation and subsequent varicose veins. • Venous leg ulcers are also correlated with increased ambulatory venous pressures. • With loss of perforator valve function, the high intracompartmental venous pressure, which can approach 200 mm Hg during active muscle contraction, results in distention of the saphenous system.



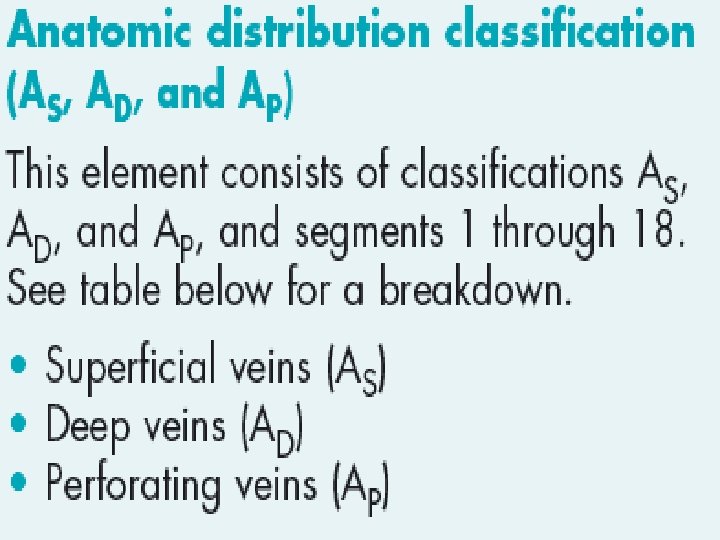
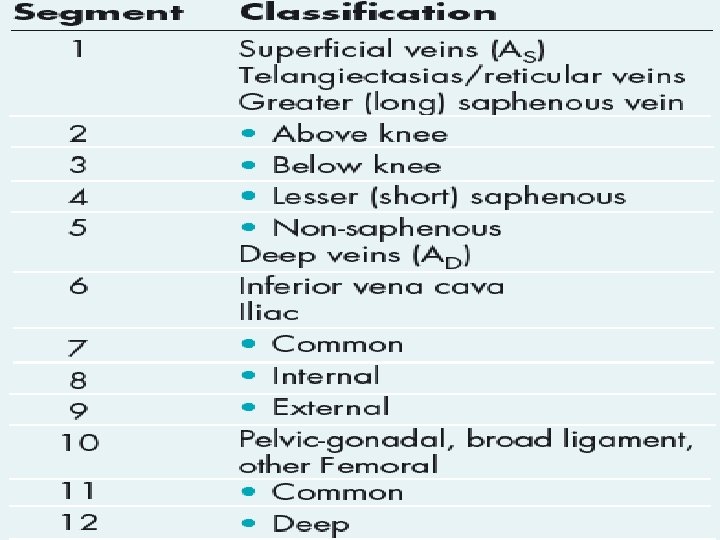
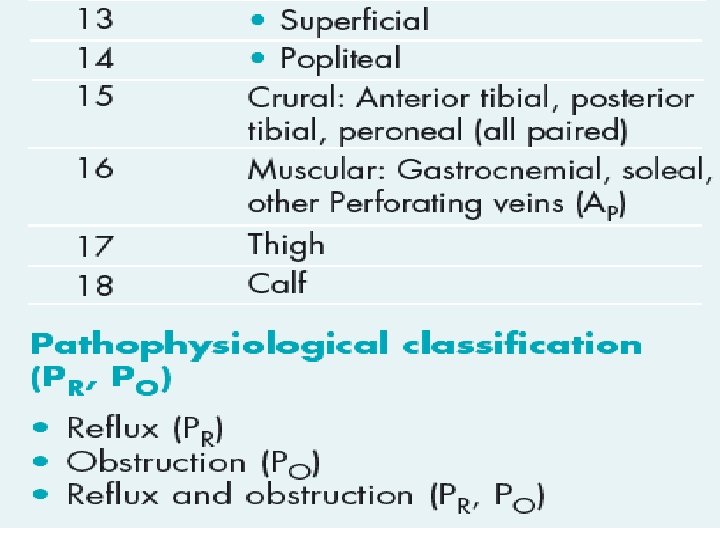
CEAP classification system • The CEAP classification system for chronic • venous disease consists of four elements: • Clinical classification • Etiologic classification • Anatomic classification • Pathophysiological classification.


DIAGNOSING VENOUS ULCERS • Physical examination • VASCULAR TESTING

Physical examination • Skin changes in venous disease include hyperpigmentation, dermatitis, lipodermatosclerosis, or atrophie blanche, a characteristic white patchy scarring at the site of previous ulcers. • The skin over varicose veins is often warmer than the surrounding skin. Patients presenting with foot or leg ulcers should be tested for neuropathy. • Early edema may be observed as a difference in calf circumference between legs and should be confirmed by measurement. After edema has been longstanding tissue fibrosis occurs. Venous signs and symptoms

Venous signs and symptoms • gradual onset of discomfort • nondescript aching • sensations in the legs include fullness, swelling, tightness, aching, or heaviness • DVT • Varicose veins occasionally produce a pulling, prickling, or tingling and claudication • The ulcer edges may be irregular with firm fibrotic and indurated surrounding skin. The surrounding tissue may have a brownish rust color due to erythrocyte breakdown and deposition of hemosiderin. • Scar tissue may indicate the site of a previous ulcer.


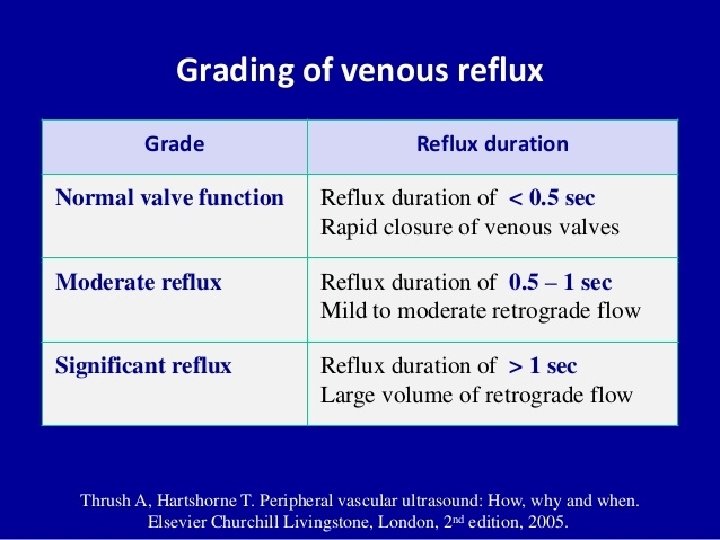
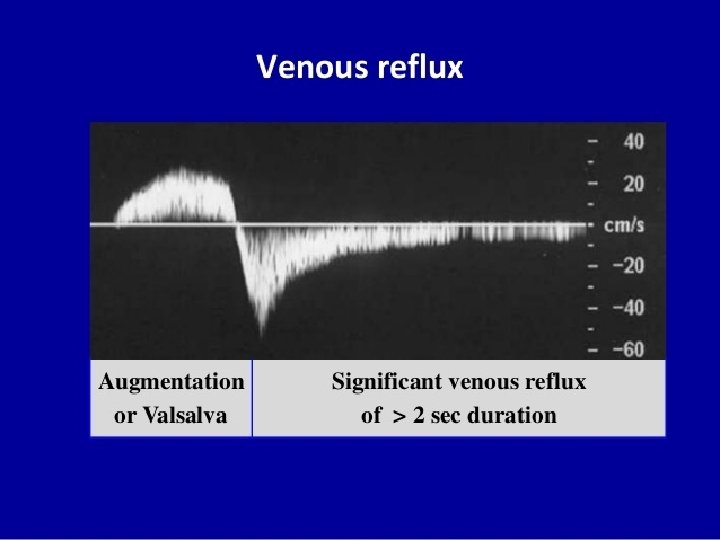
VASCULAR TESTING • Although an experienced vascular clinician can make a vascular diagnosis based on history and physical examination alone, vascular laboratory studies contribute to the accuracy of the diagnosis. • Doppler ultrasound • Duplex ultrasound • Venous testing

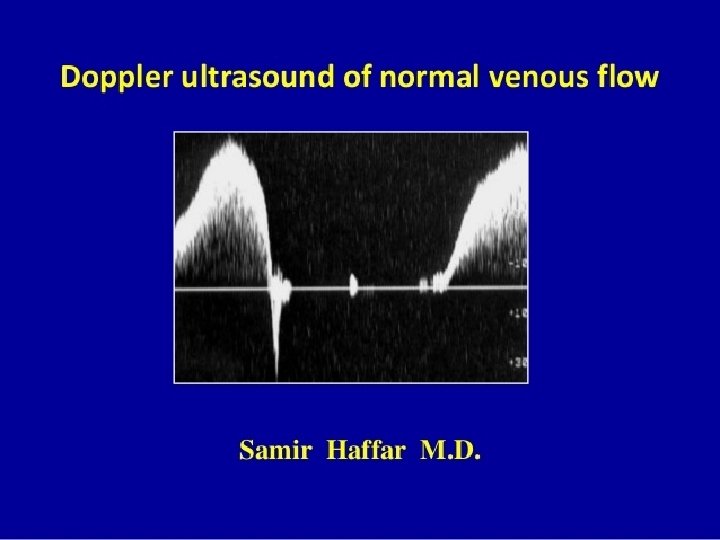
Doppler ultrasound In a Doppler ultrasound, a transmitting probe sends a signal which is reflected from an object to the receiving probe. If the signal strikes a moving object such as blood cells, a frequency shift is detected and reflected as sound. The audible signals of venous and arterial flow patterns can be distinguished.
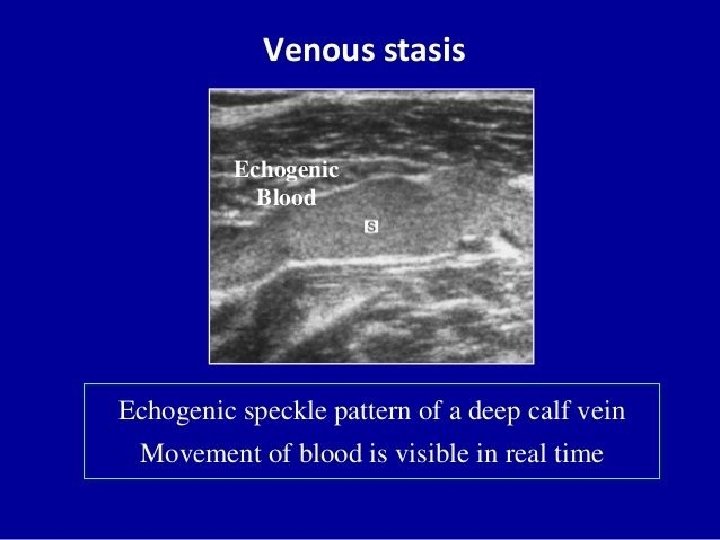

Duplex ultrasound • The advantage of venous duplex imaging is that it can identify sites of thrombosis with high levels of accuracy. • The disadvantage is that it’s fairly time consuming, taking 1 to 2 hours per evaluation for a full leg imaging.

Venous testing most commonly used to assess the severity of venous insufficiency. venous photoplethysmography (PPG). PPG, which measures the degree of light attenuation, which is proportional to the quantity of blood present and not actual volume change.

TREATING VENOUS ULCERS Treatment goals for all ulcers are to: • provide an environment conducive to new tissue growth • protect the wound • prevent further tissue destruction.

Wound infection Infected leg ulcers, soft-tissue cellulitis, and osteomyelitis are treated by administering systemic IV or oral antibiotics. Topical antibiotics are not indicated for all leg ulcers. Chronic wounds are colonized with normal skin flora and shouldn’t be treated with antibiotics. Rigorous and frequent ulcer cleansing assists in removing surface bacteria. Newer silver impregnated dressings have been effective in managing bacteria and promoting healing by keeping the wound surface clean.

Skin and wound care • A clean wound, free from dead tissue and wound debris, is necessary for healing to occur. Wound cleaning and debridement are the initial steps in wound care. Many commercial wound cleaners and disinfectants are cytotoxic. Povidoneiodine, hydrogen peroxide, and 0. 25% acetic acid have shown evidence of interfering with fibroblast formation and epithelial growth. • Hydrotherapy or whirlpool. Whirlpool may be contraindicated if the water and dependent position increase edema in the leg. • Dressings

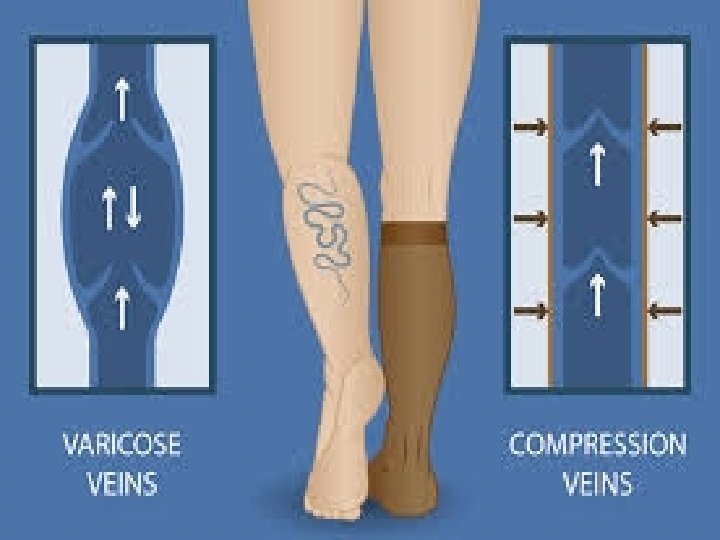
Compression • Compression is the application of pressure to the limb. It is measured in millimeters of mercury (mm Hg) and is applied by bandages, elastic stockings, and/or intermittent pneumatic compression pumps. • Elastic bandages are considered long stretch and capable of stretching to double their size. Because these dressings can be stretched too tight, they are not recommended as a primary dressing for compression. • Inelastic bandages are nonstretch bandages, short-stretch bandages, and zinc paste bandages. The resting pressure under inelastic bandages decreases over a 24 -hour period, but the working pressure (with muscle movement) decreases less. • Compression wraps should be applied starting just below the toes and ending just below (two finger breadths) the popliteal fossa.


Assessment of treatment • EXERCISE • A graded exercise program may be used to improve the calf muscle pump in those patients with abnormalities in pump function. • Effective edema removal from the leg reverses much of the associated comorbidity, particularly the skin changes. • Therapists can be very creative in combining or layering different compressive products to achieve adequate levels of compression. Compliance is crucial to prevent recurrence of edema.

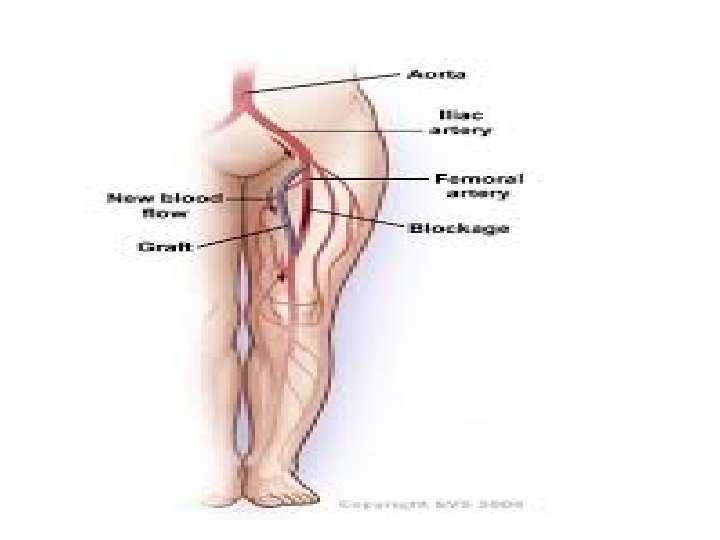
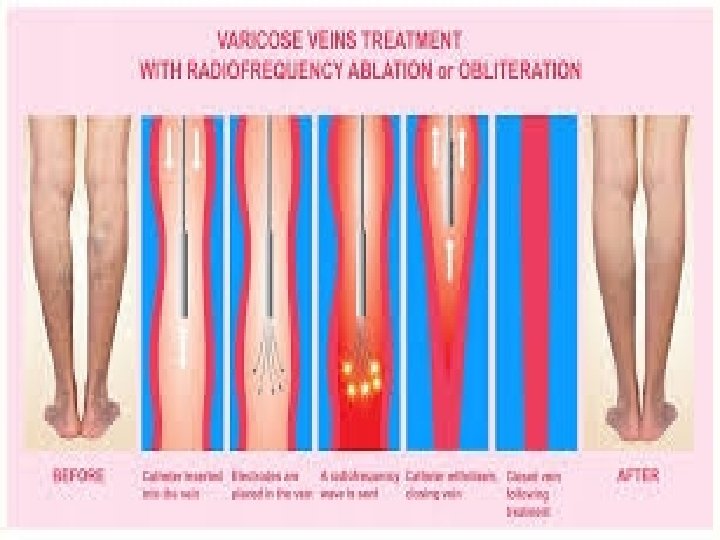
Surgical treatment for venous ulcers • Procedures aimed at correcting insufficiency of the deep venous system include vein valve transplantation, direct valve repair, and veno-venous bypass. • Outflow obstruction of a limb is addressed with venous bypass, endovascular intervention, or a combination of the two. Varicose veins, the manifestation of superficial venous insufficiency, generally require ablation. Their treatment is usually by excision, ligation, injection, or the more recent method of endovenous ablation, depending on the size of the vein.
- Slides: 40