CME Disclosure Statement The North Shore LIJ Health





 • For given α, β, p 0, and")


 • Treatment Plan • Blinding • Use of Placebo Control •")
 • Blinding • Placebo control • Stratification • The process of")


 Compliance in Group A")

 • Randomized, double-blind, placebo-controlled trial to")

- Slides: 33
CME Disclosure Statement • The North Shore LIJ Health System adheres to the ACCME's new Standards for Commercial Support. Any individuals in a position to control the content of a CME activity, including faculty, planners and managers, are required to disclose all financial relationships with commercial interests. All identified potential conflicts of interest are thoroughly vetted by the North Shore-LIJ for fair balance and scientific objectivity and to ensure appropriateness of patient care recommendations. • Course Director, Kevin Tracey, has disclosed a commercial interest in Setpoint, Inc. as the cofounder, for stock and consulting support. He has resolved his conflicts by identifying a faculty member to conduct content review of this program who has no conflicts. • The speaker, Martin L. Lesser, Ph. D, has no conflicts. 2
Phase I Designs • “ 3+3” dose escalation design for determining maximum tolerated dose (MTD) • Fixed multiple dose design (e. g. , randomize 5 subjects to each of 5 doses) • Goal: design should protect subjects from harm, especially in a trial for which safe dosing, pharmacokinetics, and potential toxicities are unknown or poorly understood
X 1=# of DLTs in first cohort of 3 X 2=# of DLTs in first cohort of 3 DLT=dose limiting toxicity Source: Jovanovic, et al. 2004
Phase II Designs • Applied to a specific disease entity • Fixed dose is used • Simple primary outcome: response, measurement of some parameter • Single arm, open label (traditional) • Single arm, blinded evaluator (uncommon) • Simon 2 -stage design • Randomized Phase II trial (for selection of best therapy)
Simon 2 -Stage Optimal Design • H 0: p ≤ p 0 vs. HA: p ≥ p 1 • Where response rate ≤ p 0 is uninteresting and response rate ≥ p 1 is the desired target • Simon’s “Optimal Design”: Observe n 1 subjects in stage 1. If response rate r 1≤ a 1/n 1, then stop the trial and reject the drug. • If r 1> a 1/n 1, then study an additional n 2 subjects in stage 2, for a total of n=n 1+n 2. If the “total” response rate r ≤ a/n, then reject the drug. If r > a/n, then consider the drug for further testing and Phase III trials. Simon: Controlled Clin Trials, 10: 1 -10, 1989.
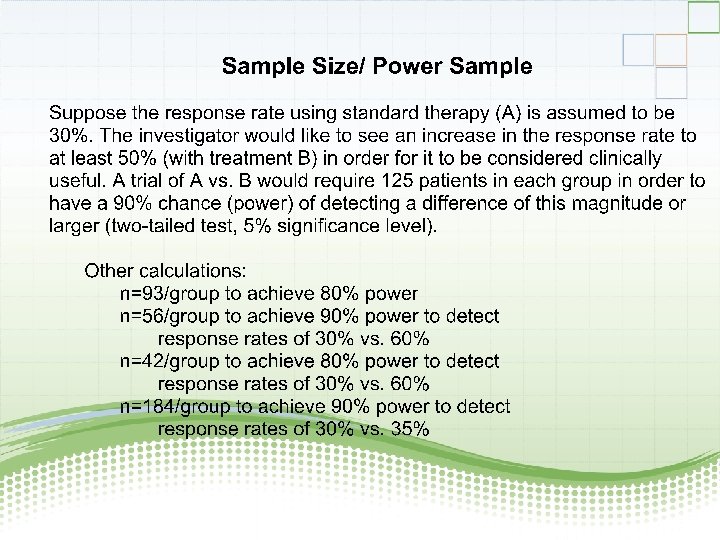
Simon 2 -Stage Optimal Design (cont’d) • For given α, β, p 0, and p 1, this design minimizes EN(p 0), the expected number of subjects studied under H 0. • Example: Let α=0. 05 β=0. 20 p 0= 0. 30 p 1= 0. 45 Stage 1: Enter 27 subjects; stop trial and reject drug if r 1≤ 9/27. If r 1 > 9/27, then go on to Stage 2: Enter 54 additional subjects (total=81). If r ≤ 30/81, then reject the drug. If r > 30/81, then trial is favorable toward drug. Note: E(N(p 0)) = 41. 7. Prob(early termination)=0. 73
Simon 2 -Stage Minimax Design • Similar to the 2 -stage optimal design • Minimizes the maximum total sample size (n) among all optimal designs • Minimax design is attractive when subject accrual is low • Previous example worked with minimax: r 1≤ 16/46, r ≤ 25/65, EN(p 0)=49. 6, PET(p 0)=0. 81 (Optimal design had n=81. )
Phase III Trials
Design Considerations (continued) • Treatment Plan • Blinding • Use of Placebo Control • Criteria for evaluation of treatment effect (comparability of patient follow-up)
Design Considerations (continued) • Blinding • Placebo control • Stratification • The process of randomization • Handling dropouts and non-compliance • Statistical methods for data analysis • Sample size and power • Interim analysis and early stopping
Blinding • Any attempt to make study participants unaware of which treatment is offered • Is indicated when the occurrence and reporting of outcomes can be easily influenced by knowledge of treatment (subjective responses, behavior change) • May be either single blind or double blind • Blinding is not always feasible • Blinding may be unsuccessful (ability to break the blind)
Placebo Control • Appropriate when no effective standard treatment exists for the control group • Makes subject’s attitudes to the trial as similar as possible in the treatment and control groups • Major uses: − Controls for psychological factors − Maintains double blind design − Controls for spontaneous disease variability • Ethical issues: - May be unethical to withhold treatment in order to administer placebo
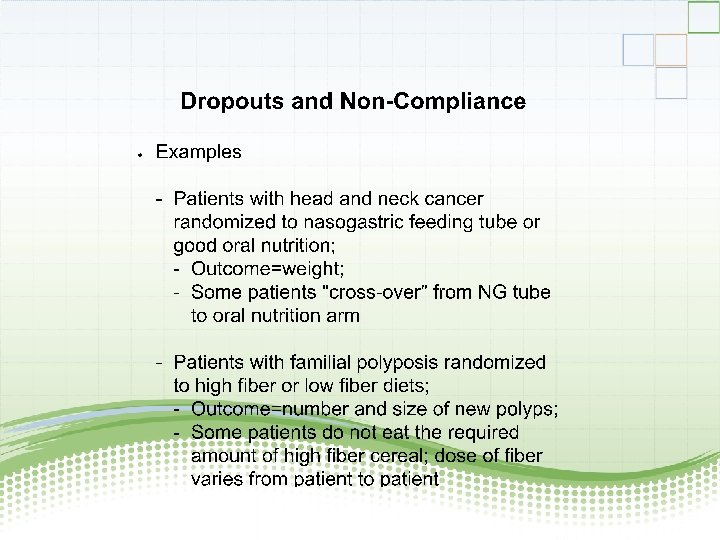
Example: RCT in Head and Neck Cancer Assuming Full (100%) Compliance in Group A Weight Gain (lbs. ) n=50 A RANDOMIZE B NG Feeding Tube µ=8. 0, σ=3 7. 57 ± 2. 84 n=50 Best Oral Nutrition µ=5. 0, σ=3 4. 61 ± 3. 01 A vs. B P<0. 0001
Example: RCT in Head and Neck Cancer Assuming 50% Compliance in Group A Weight Gain (lbs. ) n=25 A 1 n=50 RANDOMIZE A B NG Feeding Tube A 2 Pull out NG tube and default to best oral nutrition µ=4. 5, σ=3 Compliant with NG tube µ=8. 0, σ=3 Best Oral Nutrition µ=5. 0, σ=3 A 1 6. 39 ± 2. 74 A 1 A 2 n=25 n=50 5. 00 ± 2. 42 7. 78 ± 2. 34 5. 44 ± 2. 81 B 5. 66 ± 2. 98 A vs. B (ITT) A 2 vs. B A 2 vs. A 1+B A 1 vs. A 2 vs. B p=0. 2098 p=0. 0028 p=0. 0009 p=0. 0003
Example: The BHAT Trial (Beta-blocker Heart Attack Trial) • Randomized, double-blind, placebo-controlled trial to test the effect of propanolol (beta-blocker) on total mortality • n = 3837 patients randomized to propanolol or placebo • Trial was stopped 1 year early (on the 6 th interim analysis) using the O-F group sequential approach when logrank X 2 =2. 82 > 2. 23
O’Brien-Fleming Boundaries Applied to the BHAT Trial