Cardiac causes of cardiac arrest Learning outcomes This







 Airway • Assessment – patient talking – complaining of severe central")
 Breathing • Assessment • Treatment – R - RR 20 min-1")
 Circulation • Assessment – – regular radial pulse , rate 100")
 Circulation • Assessment – – – – regular radial pulse ,")
 Disability • Assessment – alert and anxious – pupils equal, react")

 Airway • Assessment – patient talking – complaining of severe central")
 Breathing • Assessment • Treatment – continue high flow oxygen –")
 Circulation • Assessment – – – Cool, clammy peripheries, regular radial")
 Circulation • Response – – troponin result - raised IV pain")
 Disability • Assessment – alert and anxious – pupils equal, react")








- Slides: 28
Cardiac causes of cardiac arrest
Learning outcomes This lecture should enable you to: • describe the different types of ACS • explain how to recognise and assess an ACS • list the relevant immediate treatment for each type of ACS • discuss how to recognise and respond to other cardiac conditions that may cause cardiac arrest
Acute coronary syndromes Clinical syndromes caused by the same disease process: • unstable angina • non-ST-elevation myocardial infarction • ST-elevation myocardial infarction
Risk Stratification Enzymes – e. g. Troponin ECG changes History
Unstable Angina NSTEMI Presenting history Normal ECG ST elevation on ECG Non specific abnormalities of the ECG ST Depression on ECG Consistently negative or small rise in troponin Troponin release New left bundle branch block Troponin release
Immediate treatment for all acute coronary syndromes ABCDE approach • • • aspirin 300 mg orally (crush/chew) consider other antiplatelet medication nitrate (GTN tablet or patients own spray) fentanyl/morphine oxygen - if hypoxic or signs of shock • (Sp. O 2 <94% or no measurement available) • Target for = Sp. O 2 94% to 98%
Case 1 Clinical setting and history I You receive a call from a nurse S asking you to review urgently a 55 -year-old woman with a 1 -hour history of central chest pain B Jasvinder self-presented and is normally well A She looks unwell, clammy and anxious R Please assess her immediately
Case 1 (continued) Airway • Assessment – patient talking – complaining of severe central chest pain, radiating to neck and down left arm There is no evidence of airway obstruction • Treatment/Action – high flow oxygen started • Response – no change
Case 1 (continued) Breathing • Assessment • Treatment – R - RR 20 min-1 – inspired oxygen concentration reduced – A - normal, symmetrical chest expansion, breath sounds • Response and percussion note – Sp. O 2 97% using 3 L min-1 via – T – trachea normal nasal prongs – E – normal effort – S - Sp. O 2 100% on high flow oxygen Her Sp. O 2 indicates that her oxygen concentration should be reduced
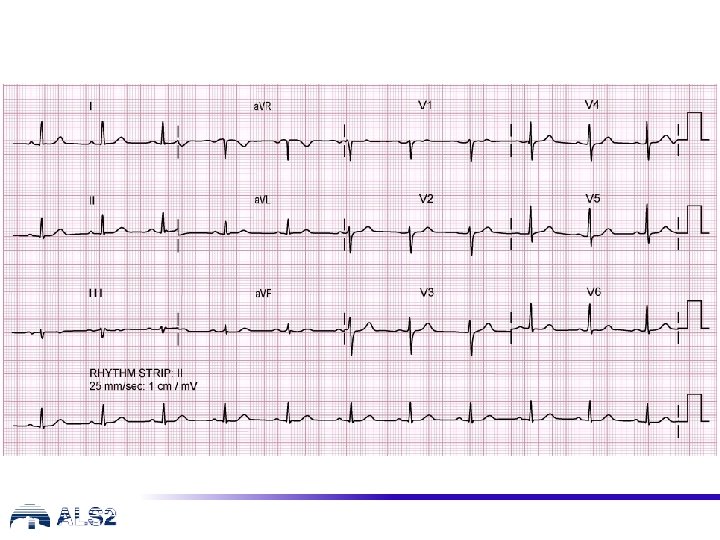
Case 1 (continued) Circulation • Assessment – – regular radial pulse , rate 100 min-1 BP 110/65 mm. Hg, CRT <2 s normal heart sounds ECG monitor • request 12 lead ECG (next slide) – bloods including troponin • Treatment/Action – – venous/vascular access aspirin to chew sublingual nitrate/GTN IV fentanyl/morphine
Case 1 (continued) Circulation • Assessment – – – – regular radial pulse , rate 100 min-1 BP 110/65 mm. Hg, CRT <2 s normal heart sounds ECG monitor request 12 lead ECG venous/vascular access bloods including troponin • Treatment/Action – aspirin to chew – sublingual GTN – IV fentanyl/morphine • Response – – reduces chest pain first troponin normal ECG - ST Depression repeat troponin later With the history and findings a likely cause is an ACS
Case 1 (continued) Disability • Assessment – alert and anxious – pupils equal, react to light – blood glucose 7. 0 mmol L-1 • Treatment/Action – nil • Response – no change Exposure • Assessment – no bleeding or rashes – temperature 36. 6 ˚C • Treatment/Action – nil • Response – no change Plan: Requires urgent cardiology review (? Unstable Angina/NSTEMI) awaiting repeat troponin - consider oral anti-platelets and anticoagulation also pain relief and myocardial protection
Case 2 Clinical setting and history I You are called to assess a patient by a colleague S A 63 year old gentleman with a 1 -hour history of central chest heaviness and shortness of breath B Bill was sitting at his desk when the pain started, similar to his angina, but unrelieved by GTN spray A He looks unwell, clammy and anxious R Please assess him immediately
Case 2 (continued) Airway • Assessment – patient talking – complaining of severe central chest pain (heaviness) – no evidence of airway obstruction • Treatment/Action – high flow oxygen started • Response – no change
Case 2 (continued) Breathing • Assessment • Treatment – continue high flow oxygen – R - RR 23 min-1 – A - bilateral basal crackles, • Response symmetrical chest expansion – Sp. O 2 remains unrecordable – S - Sp. O 2 not able to be recorded on high flow oxygen – T - normal – E - increased effort Inability to record Sp. O 2 indicates that high flow oxygen concentration should be used
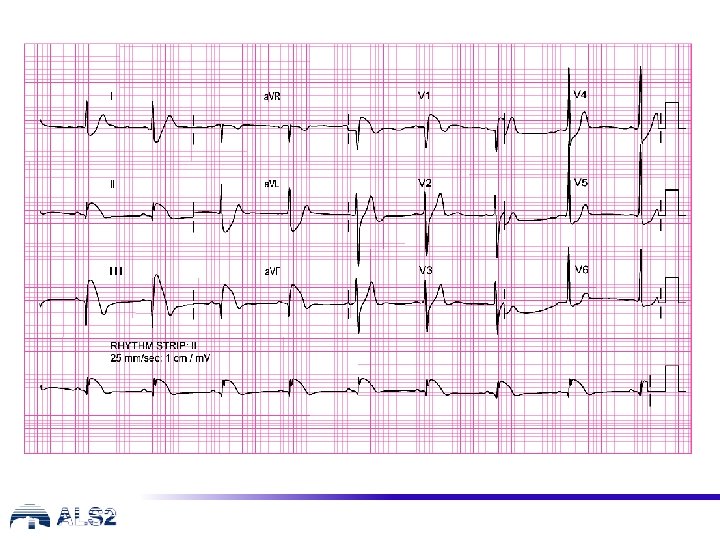
Case 2 (continued) Circulation • Assessment – – – Cool, clammy peripheries, regular radial pulse , rate 55 min-1 BP 80/65 mm. Hg, (right = left arm) CRT 4 s normal heart sounds request 12 lead ECG • Treatment/Action – aspirin to chew – IV access obtained – blood samples taken • including troponin – IV fluid commenced – IV fentanyl/morphine – sublingual GTN Expert help cardiology/resuscitation team With the history and findings the most likely cause is an ACS
Case 2 (continued) Circulation • Response – – troponin result - raised IV pain relief reduces chest pain ECG (Inferior STEMI) Plan for reperfusion With the history and findings the most likely cause is a STEMI
Case 2 (continued) Disability • Assessment – alert and anxious – pupils equal, react to light – blood glucose normal • Treatment/Action – nil • Response – no change Exposure • Assessment – – clammy, sweating and pale ankle oedema no bleeding or rashes Temperature 36. 3 ˚C • Treatment/Action – nil • Response – no change Plan: STEMI – emergency reperfusion
Access to emergency reperfusion
Other cardiac causes of cardiac arrest • in any cardiac arrest look for evidence of the cause • not all cardiac arrests are due to ACS • other causes may be ‘structural’ or ‘electrical’ • some are inherited, some acquired, some congenital
Examples of other cardiac causes Condition Nature Causation Severe aortic stenosis Structural Mostly acquired Sometimes congenital Hypertrophic cardiomyopathy Structural Inherited High-grade AV block Electrical Mostly acquired Occasionally congenital Long QT syndrome Electrical Inherited, but… there are other causes of a long QT interval Anomalous coronary anatomy Structural Congenital
Long QT syndrome
Other cardiac causes: preventing cardiac arrest • be alert for warning symptoms (e. g. unexplained syncope) • arrange urgent specialist assessment and treatment (including genetic family) • with inherited conditions, don’t forget the family
Any questions?
Summary • • • recognise the different presentations of ACS use the ABCDE approach start appropriate immediate treatment arrange immediate PPCI when appropriate be aware of other cardiac causes of arrest requiring different management
Advanced Life Support Level 2 Course Slide set All rights reserved © Australian Resuscitation Council (August 2018)