Advances and Controversies in Cardiovascular Risk Prediction Promises











 2004")
























- Slides: 37
Advances and Controversies in Cardiovascular Risk Prediction Promises, Pitfalls and Progress Peter Brindle General Practitioner R&D lead Bristol, N. Somerset and S. Glouc PCTs
Outline • Promises – Why do CVD risk estimation? – Background – Framingham • Pitfalls – How well to current methods perform? – Two studies • Progress – Four new risk scores – Where to next?
PROMISES
Why do CVD risk estimation? • To identify high risk individuals • Prioritise treatment - for individuals - for policy • Patient education
Background • Guidelines recommend preventive treatment in high risk patients • Population screening • Lifelong treatment. Or not.
The Framingham Heart Study • Data collection started in 1948 • Bi-annual follow up • First CVD risk equation: Truett et al. 1967 • > 20 groups of regression equations between 1967 and 2008 • Modified Anderson et al 1991 used in UK
Framingham - Anderson • Data collected 1968 -75 • 5573 men and women followed up for 12 years • Six regression equations published in 1991
Risk factors used to calculate the Anderson Framingham risk score -age and sex -diastolic and systolic BP -total: HDL cholesterol ratio -diabetes (Y/N) -cigarette smoking (Y/N) -LVH (Y/N) Absolute CVD Risk over 10 years
Different versions and coloured charts New Zealand cardiovascular risk prediction charts
Sheffield Tables
Joint British Societies 1998
Joint British Societies(2) 2004
PITFALLS
Getting it wrong Over-prediction means. . . People with little to gain may become patients, and the benefit to risk ratio of treatment becomes too small Under-prediction means… People with much to gain may not be offered preventive treatment
How well does Framingham perform? • Single UK population • One systematic review
Framingham in the Renfrew/Paisley study § 12, 300 men and women, aged 45 -64 and no evidence of cardiovascular disease at entry (1972 -76) § 10 -year follow up for cardiovascular disease mortality § Stratified by individual social class and area deprivation
Social deprivation 10 -year predicted versus observed CVD death rates by area deprivation and social class Social class Deprivation (Pred/Obs) Non-Manual 0. 69 Manual 0. 52 p= 0. 0005 Affluent 0. 64 Intermediate 0. 56 Deprived 0. 47 p= 0. 0017 for trend The Framingham risk score does not reflect the increased risk of people from deprived backgrounds relative to affluent people
Predicted over observed ratios ordered by background risk of test population
Issues with Framingham • • BP treatment Family History Deprivation Ethnicity Generalisability Statistical validity Face validity Improvements are needed
PROGRESS
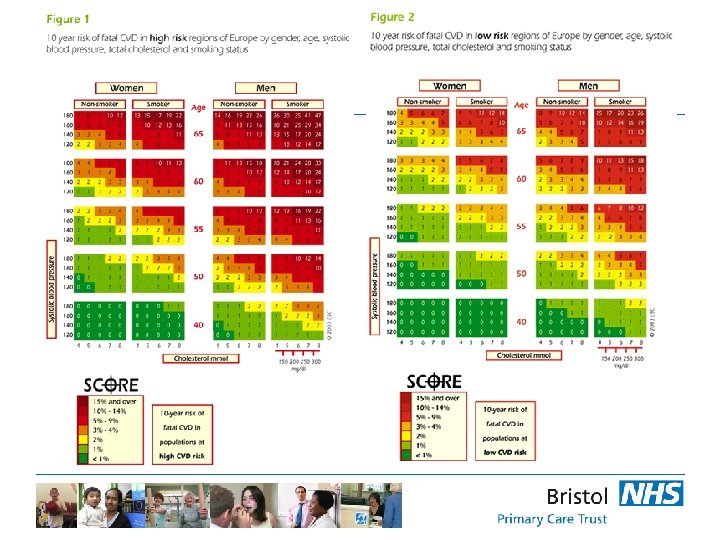
SCORE Systematic Coronary Risk Evaluation 2003 • 205, 178 men and women from 12 European cohort studies • Used by “European guidelines on cardiovascular disease prevention in clinical practice”
SCORE – better than Framingham? SCORE BP treatment Family History Deprivation Ethnicity Generalisability Statistical validity Face validity No No ? Yes No
ASSIGN - ASSessing cardiovascular risk, using SIGN guidelines • Scottish Heart and Health Extended Cohort (SHHEC) • 6540 men, 6757 women • Classic risk factors plus – Deprivation – Family history • Shifts treatment towards the socially deprived compared to Framingham
ASSIGN – better than Framingham? SCORE ASSIGN BP treatment No No Family History No No Yes No ? Yes No Deprivation Ethnicity Generalisability Statistical validity Face validity
QRISK 1 and QRISK 2 • Electronic patient record • Cohort analysis based on large validated GP database (QResearch) • Contains individual patient level data • 15 year study period 1993 to 2008 • First diagnosis of CVD (including CVD death) • QRISK 1 – – § Deprivation Family History BMI On BP treatment NO Ethnicity
QRISK 1 - better than Framingham? BP treatment Family History Deprivation Ethnicity Generalisability Statistical validity Face validity SCORE ASSIGN QRISK 1 No No ? Yes No No Yes No ? Yes No Yes Yes Yes
QRISK 2 • • • Included ONS deaths linkage Included additional variables 2. 3 million people (>16 million person yrs) Self-assigned ethnicity Derivation (1. 5 million) and test cohorts
Model performance QRISK 2 vs Modified Framingham QRISK 2 Framingham R squared 43. 4% 38. 9% D statistic 1. 793 1. 632 R squared 38. 4% 34. 8% D statistic 1. 616 1. 495 Females Males
Age-standardised incidence of CVD by deprivation
Adjusted Hazard Ratios for CVD
QRISK 2 – better than Framingham? BP treatment Family History Deprivation Ethnicity Reproducibility Generalisability Statistical validity Face validity SCORE ASSIGN QRISK 1 QRISK 2 No No Yes ? Yes No No Yes ? Yes No Yes Yes Yes Yes
Where to next? • Generalisability? • Linkage – Census – Hospital data • Improved ethnicity recording
Summary • Promises – Why do CVD risk estimation? – Background – Framingham • Pitfalls – How well to current methods perform? – Two studies • Progress – Four new risk scores – Where to next? – linkage and statistics
CONCLUSION • The idea of risk assessment is well established • Existing methods flawed – but better than nothing • Electronic patient record + improving data sources = exciting prospects
Acknowledgements • British Regional Heart study team • Renfrew/Paisley study team • Shah Ebrahim • Tom Fahey • Andy Beswick • Julia Hippisley-Cox • John Robson • Carol Coupland • Yana Vinogradova • Aziz Sheikh • Rubin Minhas
CONCLUSION • The idea of risk assessment is well established • Existing methods flawed – but better than nothing • Electronic patient record + improving data sources = exciting prospects