ACUTE VIRAL HEPATITIS Dr Akhavan Clinical Manifestations The









,")











- Slides: 23
ACUTE VIRAL HEPATITIS Dr. Akhavan
Clinical Manifestations • The clinical manifestations of acute viral hepatitis are similar among the five hepatitis viruses • Asymptomatic infections with the hepatitis viruses are approximately 10 to 30 times more common than symptomatic ones.
Clinical Manifestations • Approximately 25% of patients report the onset of symptoms as a “flulike” illness. • malaise, fatigue, myalgia, arthralgia, and headache. Anorexia, nausea, and vomiting may occur, sometimes associated with alterations in olfaction and taste. • Pharyngitis, coryza, and cough may also be present. • Low-grade fever is common and more frequent in hepatitis A and E, rather than in hepatitis B or C, except when hepatitis B is associated with a serum sickness–like syndrome, in which a fever of 39. 5° C to 40° C may be present
Clinical Manifestations • Dark urine and clay-colored stools may appear, usually 1 to 5 days before the onset of icterus • Right upper quadrant tenderness • Splenomegaly and cervical lymphadenopathy are seen in 10% to 20% of patients.
Clinical Manifestations • With the onset of jaundice, the constitutional symptoms generally abate but may continue during the entire icteric period. • The duration of the posticteric phase is variable and ranges from 2 to 12 weeks • Complete resolution of clinical and laboratory abnormalities is to be expected 3 to 4 months after the onset of jaundice in 75% of cases of uncomplicated acute hepatitis B or C.
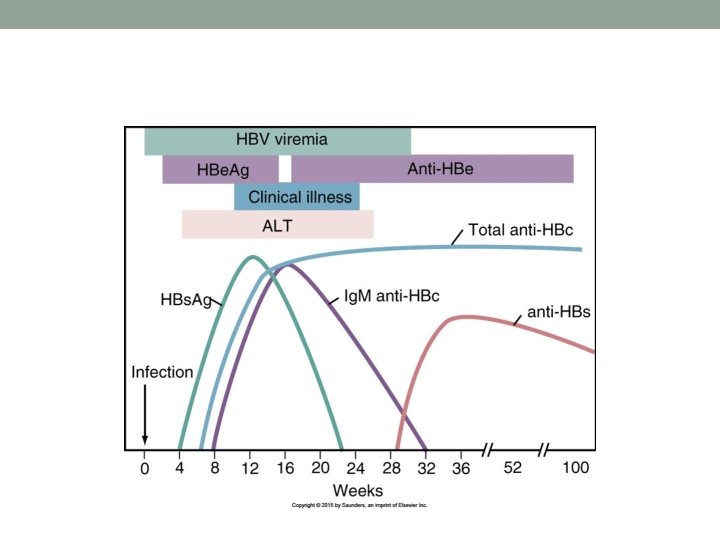
Prognosis of Acute Hepatitis • 95% to 99% of otherwise healthy, immunocompetent patients with acute hepatitis B recover completely.
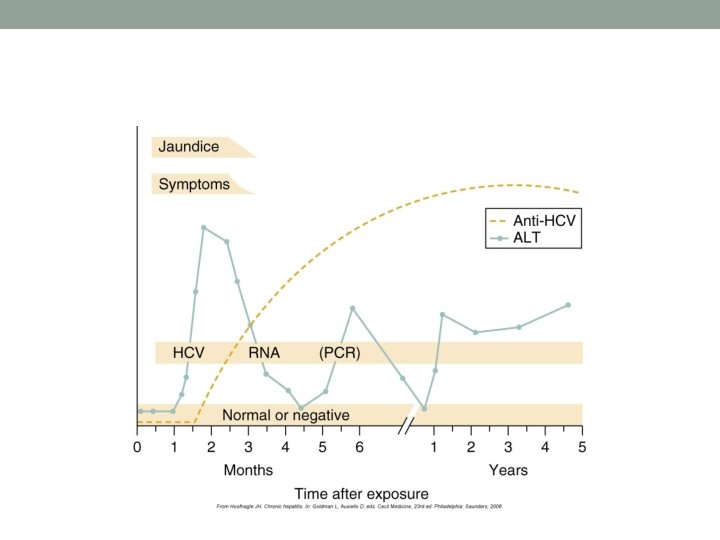
Prognosis of Acute Hepatitis • chronic hepatitis C follows acute infection in approximately 85% of cases • acute hepatitis B and acute hepatitis D do not necessarily have a more severe disease • In contrast, hepatitis D superinfection of established chronic hepatitis B infection often leads to clinical deterioration
more complicated and protracted courses of acute viral hepatitis 1. 2. 3. 4. 5. 6. 7. 8. 9. advanced age serious underlying medical conditions. ascites, peripheral edema, hepatic encephalopathy prolonged prothrombin time, low serum albumin, hypoglycemia, very high serum bilirubin
Fulminant Hepatitis • severe liver failure developing within 8 weeks of the onset of symptoms • usually present with hepatic encephalopathy, which may evolve into a deep coma. Liver size is reduced, bilirubin rises, and prothrombin time is markedly prolonged, even as aminotransferase levels drop. Ascites and peripheral edema are present, consistent with hepatic failure.
Fulminant Hepatitis • The mortality rate is high (>80% in patients with deep coma), but those who survive have a complete clinical and laboratory recovery. • Liver transplantation, if it can be performed in time, may be lifesaving in such patients.
Complications of Acute Hepatitis • relapsing hepatitis • protracted cholestatic • arthritis or arthralgias, rash, angioedema, and, rarely, hematuria and proteinuria. • Essential mixed cryoglobulinemia • associated lymphoproliferative disorders can complicate chronic (not acute) hepatitis C, • hepatitis C may be associated with abnormalities in lipoprotein and glucose metabolism. • The risk of chronic infection after acute hepatitis B in otherwise healthy adults is appropriately 1%, whereas the corresponding risk of chronicity after acute hepatitis C is 85% to 90%. • Both chronic hepatitis B and C are associated with an increased risk of hepatocellular carcinoma
DIAGNOSTIC INTERPRETATIO N SEROLOGIC TESTS OF PATIENT’S SERUM HBs. Ag Ig. M Anti-HAV Ig. M Anti-HBc Anti-HCV Acute hepatitis B + − Chronic hepatitis B + − − − Acute hepatitis A superimposed on chronic hepatitis B + + − − Acute hepatitis A and B + + + − Acute hepatitis A − + − − + Acute hepatitis A and B (HBs. Ag below detection threshold) Acute hepatitis C HAV, hepatitis A virus; HBc, hepatitis B core; HBs. Ag, hepatitis B surface antigen; HCV, hepatitis C virus.
Chronic Viral Hepatitis • The term chronic viral hepatitis is used to describe protracted hepatocellular necrosis and inflammation, often with fibrosis, that lasts longer than 6 months and is caused by HBV, HCV, HBV-associated HDV, or HEV
Clinical Manifestations • fatigue and, less commonly, right upper quadrant discomfort or “fullness. ” • More severe and advanced cases can be associated with fatigue and jaundice, but persons with compensated cirrhosis may have no symptoms at all. • Decompensated cirrhosis may be accompanied by fatigue, jaundice, loss of muscle mass (weight loss), ascites, edema, bruising (coagulopathy), gastrointestinal bleeding (gastroesophageal varices or portal hypertensive gastropathy), and hepatic encephalopathy.
Clinical Manifestations HBV • immune-complex manifestations, including cutaneous vasculitis, arthritis, glomerulonephritis, and generalized vasculitis
• The biochemical hallmark of chronic hepatitis B is elevation of serum aminotransferase activity, with normal to near-normal alkaline phosphatase activity. • In severe, progressive, and decompensated chronic hepatitis B, bilirubin levels can increase (hepatic excretory dysfunction), albumin can fall, prothrombin time can become prolonged (hepatic synthetic defect), and hypersplenism can occur (primarily thrombocytopenia and leukopenia).
Chronic Hepatitis D • Clinical features of chronic hepatitis D are similar to those of chronic hepatitis B, except for the increased severity and more rapid progression to cirrhosis and end-stage liver disease; in addition, both early mortality and the risk of HCC are increased in patients with hepatitis D
Chronic Hepatitis D • Serologically, the diagnosis of hepatitis D is established by the presence of circulating antibody to HDV (anti-HDV)
Chronic Hepatitis C • The most typical patient with recently discovered hepatitis C is asymptomatic, but fatigue is one of the more common clinical features in symptomatic persons.
Chronic Hepatitis C • Overall, clinical features of chronic hepatitis C, and of decompensated cirrhosis associated with hepatitis C, are similar to those of chronic hepatitis B. Laboratory test abnormalities in chronic hepatitis B and C are similar
Chronic Hepatitis C • Chronic hepatitis C can be accompanied by circulating autoantibodies, including nuclear antibodies, especially liver-kidney microsomal antibody (anti-LKM 1), similar to that seen in autoimmune hepatitis type 2