A COMPARATIVE ANALYSIS OF ANTIMULLERIAN HORMONE AND FOLLICLE


 determines prognostic chances of fertility treatments and")
, the identification of variables able to predict")
 o optimal fertility ------ 4. 0 – 6. 8 o")
 • • Very low Reserve ----- <2 Satisfactory --------- 3")























- Slides: 36
A COMPARATIVE ANALYSIS OF ANTI-MULLERIAN HORMONE AND FOLLICLE STIMULATING HORMONE IN ASSESSMENT OF OVARIAN RESERVE Dr. Kenneth Egwuda MBBS, PGA-ART(Lon), ESGE(Belg. ), FMAS, FWACS, FMC OG
Authors Egwuda, K. ; Onuh, SO. ; Ekwempu, CC. ; Shuaibu, SI. , Kamolideen, AA; Ojima, SC
AMH/FSH • A patient's ovarian reserve (OR) determines prognostic chances of fertility treatments and her treatment options • Best possible assessments of OR, therefore, represent a core issue in modern infertility care
OR • In human in-vitro fertilization (IVF), the identification of variables able to predict ovarian responsiveness to exogenous gonadotropins guides the clinician on individualizing treatment protocols, optimizing results and reducing complications
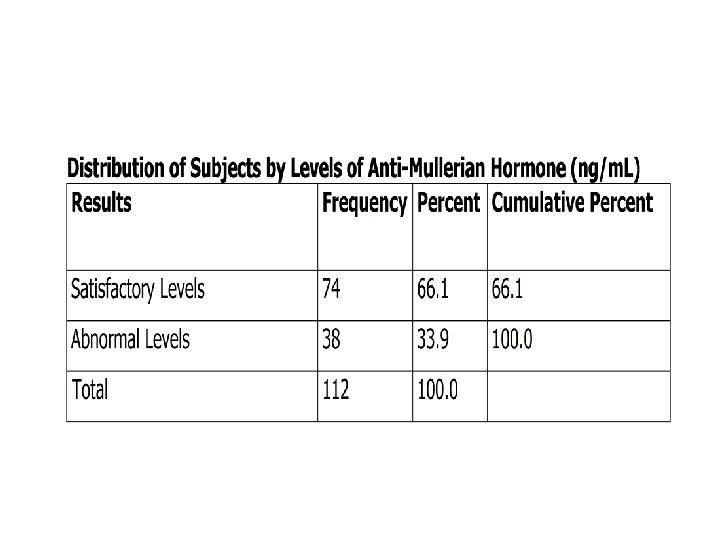
AMH Value Ranges (ng/ml) o optimal fertility ------ 4. 0 – 6. 8 o Satisfactory fertility ---- 2. 2 – 4. 0 o Low fertility --------- 0. 3 – 2. 2 o Very low fertility ------ 0. 0 – 0. 3 o High level----------- >6. 8 3/8/2021 AMH VS FSH IN OR 5
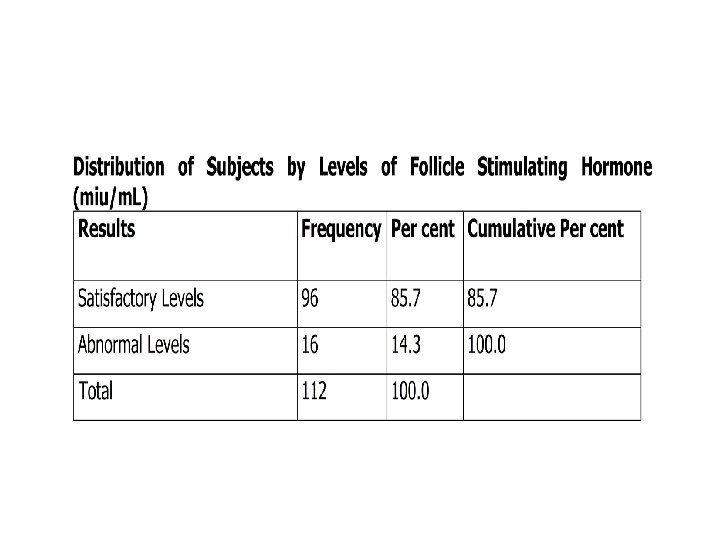
FSH Value Range (miu/ml) • • Very low Reserve ----- <2 Satisfactory --------- 3 - 10 Depleted ----------- ≥ 12 Ovarian failure ------- ≥ 25
objectives • To evaluate basal anti-müllerian hormone as compared to follicle stimulating hormone as a marker for ovarian reserve and responsiveness
Objective • To determine whether AMH is a better marker of ovarian reserve and responsiveness than FSH
Study Type • This was a hospital based study that was carried out in Fertile Aid Clinic, DEDA Hospital Abuja and a private hospital in Jos
Study Population • The study population comprised of clients who had the indication for In-vitro fertilization and Embryo Transfer (IVF-ET) or Assisted Reproductive Technology (ART), had been counselled, consented and scheduled for a treatment cycle
STUDY DESIGN • This was a cross-sectional and comparative study
INCLUSION CRITERIA • < 40 years, • having regular, menstrual cycles every 21– 35 days • having both ovaries present • no current or past diseases affecting ovaries, gonadotrophin, sex steroid secretion, clearance or excretion • they were also not on any form of hormonal therapy • their ovaries were adequately visualized at transvaginal ultrasound scanning
ETHICAL CONSIDERATION • This study was approved by the Research and Ethical Committees of the institution where it was conducted and the Federal Capital Development Authority. Informed consent was obtained from the clients before enrolment into the study. The laboratory analysis of baseline serum Anti-Mullerian Hormone was paid for by the researchers
methodology • Stored basal menstrual cycle day three serum samples of 112 women was evaluated for AMH and FSH and compared to the number of oocytes retrieved • A correlation analysis, ROC curve and analysis of variance were performed to determine the level of accuracy between AMH and FSH in predicting the ovarian reserve and responsiveness
OUTCOME MEASURED • total number of follicles ≥ 17 mm in diameter before administration of h. CG • the total number of oocytes retrieved • AMH levels • FSH levels • Duration of stimulation • Age • BMI
AMH/FSH • For the purpose of this study, serum AMH levels <2. 2 ng/ml shall be taken as an abnormal level while serum levels >2. 2 ng/ml is satisfactory. Serum FSH levels between 3 -10 miu/ml will be regarded as normal/satisfactory while levels >10 miu/ml will be regarded as abnormal
Characteristics Age Minimum Maximum Mean Std. Deviation 20 45 31. 3 6. 7 Parity 0 3 0. 5 0. 8 Weight 55. 2 117. 4 78. 8 13. 8 Height 1. 5 1. 8 1. 6 0. 1 BMI 20. 9 45. 9 29. 5 5. 2 FSH 2. 1 17. 8 5. 9 2. 6 LH 0. 3 17. 3 5. 2 3. 1 AMH 0 16. 6 3. 7 3. 0 AFC 1 22 10. 4 5. 5 before HCG 1 20 5. 5 3. 5 Number of Oocytes 0 20 7. 5 5. 2 Amp 2 6 3. 5 1. 4 Duration of Stimulation 4 15 9. 9 1. 7 Total Dose 300 5850 2583. 4 1136. 5 TABLE: 1 Characteristics of Subjects Number of Follicles ≥ 17 mm
≤ 3 Oocytes Variable AUC SE 95% CI >3 Oocytes P-Value AUC SE 95% CI P-Value Age 0. 162 0. 049 0. 067, 0. 257 0. 0001 0. 838 0. 049 0. 743, 0. 933 0. 002 BMI 0. 337 0. 070 0. 199, 0. 476 0. 034 0. 663 0. 070 0. 524, 0. 801 0. 034 FSH 0. 228 0. 064 0. 103, 0. 353 0. 0002 0. 772 0. 064 0. 647, 0. 897 0. 0003 0. 906 0. 038 0. 832, 0. 980 0. 0003 0. 094 0. 038 0. 020, 0. 168 0. 0002 AMH
Receiver operative xtic curve
COMPARISON OF PERFORMANCE OF KEY VARIABLES • It was observed that for the prediction of ≤ 3 oocytes (poor response), Anti-Mullerian Hormone provided the largest Area Under the Curve (AUC) with a value of 0. 91 on the Receiver Operating Procedure Curve, which implied an excellent balance of sensitivity and specificity for the number of oocytes ≤ 3 (P<0. 05) relative to FSH which showed AUC of 0. 228; P<0. 05
ROC
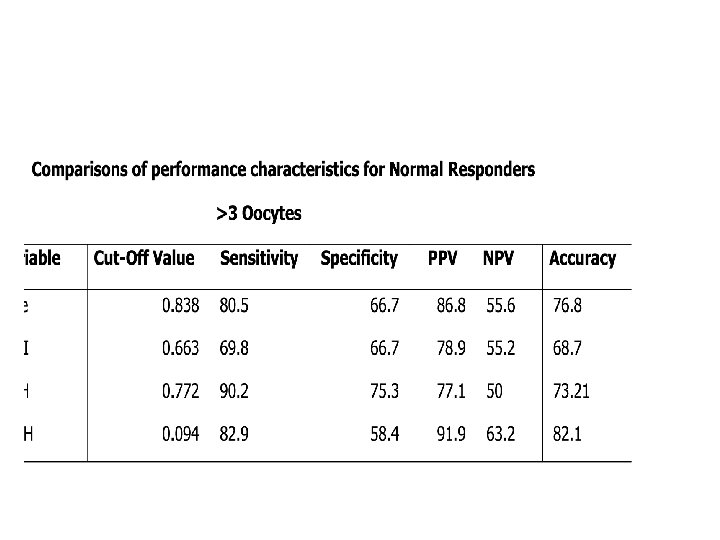
Degree of accuracy
AMH/FSH • FSH show a higher level of sensitivity for levels of Oocyte >3 oocytes retrieved. Interestingly, AMH showed a higher overall accuracy (82. 1%) even for normal responders
Multiple Linear Regression Model
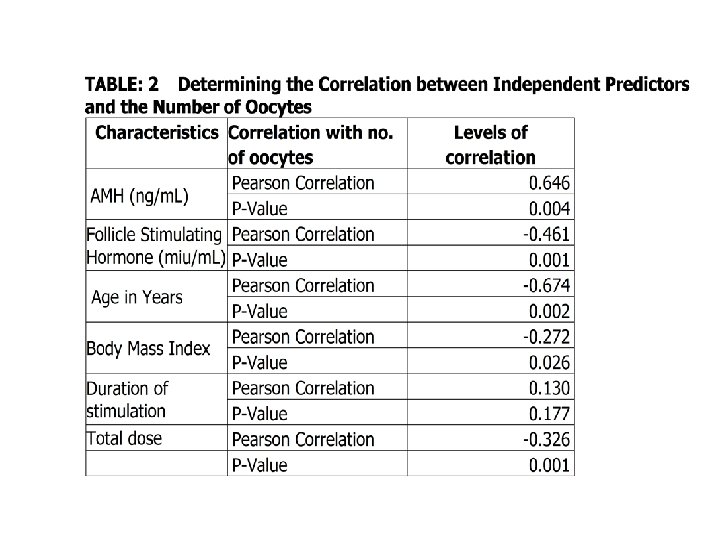
model • A model developed based on the different variable that could predict the number of oocytes retrieved in an IVF treatment cycle. Though the model looks positive, AMH appeared to be the only significant predictor of the number of oocytes retrieved as compared to other independent variables including FSH. Anti. Mullerian Hormone was also seen to have the largest contribution (4. 210) to the model since it has the highest coefficient of 0. 538
conclusion • Conventional evaluation of ovarian reserve requires specific menstrual cycle day serum evaluation of oestradiol, FSH, and LH. The accuracy of these analytes may be decreased dramatically by exogenous hormone (gonadotropin-releasing hormone agonists, gonadotropin-releasing hormone antagonists, hormonal contraceptives), endogenous hormones (elevated oestradiol levels because of a functional ovarian cyst), and timing of sample acquisition
conclusion • studies have shown that AMH results are not influenced significantly by menstrual cycle day, oestradiol, contraceptives, or gonadotropinreleasing hormone agonists. Because AMH offers added convenience and its predictive value parallels or exceeds conventional analytes testing with FSH, age, and inhibin B, AMH appears to represent a compelling tool for the assessment of ovarian reserve. Use of AMH testing is likely to improve ovarian reserve assessment in infertile patients.
conclusion Thank you