Urinary System Disorders Incontinence and Retention Loss of



 – Blood (hematuria) • Small, microscopic")


 • Very common • Urine")



 • Increase fluid intake – Especially cranberry juice • Tannin")










- Slides: 23
Urinary System Disorders
Incontinence and Retention • Loss of voluntary control of bladder • Stress incontinence – Increase in intra-abdominal pressure • Forces urine through sphincter – Laughing – Coughing – Females weakened • Spinal cord injuries, brain damage • Inability to empty bladder • May accomp overflow incontinence • Spinal cord injury • Inability to control managed by pads, briefs • Catheter – Tube inserted in urethra – Drains urine from bladder to collecting bag – Common source of UTI
Diagnostic Tests—Urinalysis • Constituents, characteristics of urine vary w/ dietary intake, drugs, care of specimen • Normally clear, straw-colored; p. H 4. 5 -8. 0 • Appearance – Cloudy • Presence of lg amts protein, blood cells, bacteria, pus – Dark color • Hematuria (blood), excessive bilirubin, high concentration of urine – Unpleasant, unusual odor • infection
Diagnostic Tests—Urinalysis • Abnormal constituents (high in numbers) – Blood (hematuria) • Small, microscopic amts – Infection, inflammation, tumors of UT • Lg # RBC – Increased glomerular permeability or hemorrhage in tract – Protein (Proteinuria) • Leakage of albumin into filtrate – Inflammation, increased glomerular permeability – Bacteria (Bacteriuria) and Pus (Pyuria) • Indicates UTI – Urinary casts • Microscopic mold of tubules – Consists of one or more cells, bacteria, protein • Inflammation of tubules – Specific gravity • Ability of tubules to concentrate urine • Low is related to renal failure
Diagnostic Tests—Blood Tests • High serum urea and creatinine – Indicate failure to excrete N wastes • Due to low GFR • Metabolic acidosis – Indicates low GFR, failure of tubules to control acid/base balance • Anemia – Indicates low erythropoietin secretion and/or bone marrow depression • Due to accumulating wastes • Electrolytes • Antibody level – Antistreptolysin O (ASO) or antistreptokinase (ASK) • Renin levels – Indicate cause of hypertension
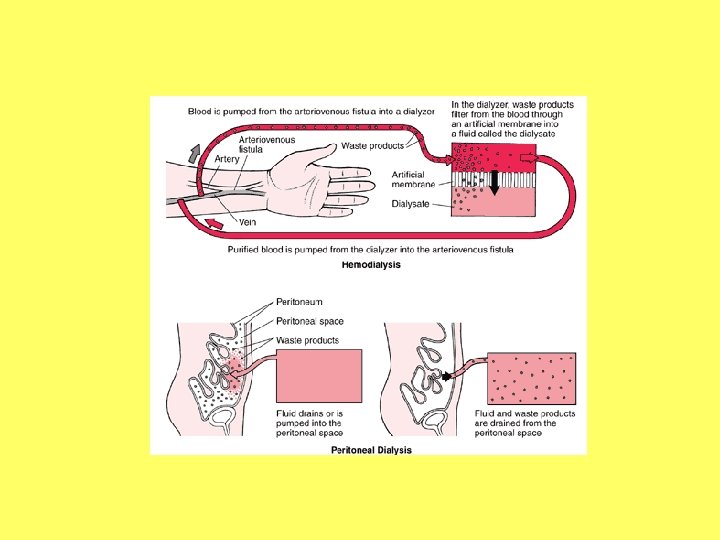
Dialysis • Provides “artificial kidney” – Sustains life after kidney fails • Acute renal failure or end-stage renal failure (those waiting for a transplant) • 2 forms – Hemodialysis – Peritoneal dialysis
Disorders of the Urinary System: Urinary Tract Infections (UTI) • Very common • Urine is excellent medium for microorganismal growth – Escherichia coli • Most are ascending – Perineal cavity mucosa bladder ureters kidneys
UTI—Etiology • Females more anatomically vulnerable – Short urethra – Proximity to anus – Frequent irritation to tissues • Tampons, bubble bath, sexual activity • Older males with prostatic hypertrophy and retention of urine prone to UTI
UTI: Cystitis—Signs and Symptoms • Pain in lower abdomen • Dysuria, frequency, urgency – Inflammation of bladder wall irritated by urine • Systemic signs of infection • Cloudy urine with unusual odor • Urinalysis indicates bacteria (+100, 000/m. L), pyuria, microscopic hematuria
UTI: Pyelonephritis—Signs and Symptoms • Signs of cystitis • Pain – Dull aching in lower back – Results from renal capsule stretching • Urinalysis – Similar to cystitis – Except urinary cast • Leukocytes or renal epithelial cells present – Involvement of renal tubules
UTI—Treatment • Antibiotics (Bactrim) • Increase fluid intake – Especially cranberry juice • Tannin decreases ability of E. coli to adhere to bladder mucosa • Infection reoccurs unless predisposing factors removed
Disorders of the Urinary System: Inflammatory Disorders • Glomerulonephritis – Many forms • Acute Poststreptococcal Glomerulonephritis (APSGN) – Follows streptococcal infection » Originates as upper resp infection, middle ear infection, strep throat – Primarily affects kids 3 -7 (especially boys) – develops 2 weeks after previous infection
Glomerulonephritis—Signs and Symptoms • Back pain – Stretching renal capsule • Dark, cloudy urine • Oliguria • Facial edema, then generalized – Low osmotic pressure of blood – Salt, water retention • Generalized signs of inflammation • Increased bp
Glomerulonephritis—Diagnostic Tests • Blood tests – High serum urea and creatinine and decreasing GFR – Streptococcal antibodies, ASO, ASK – Metabolic acidosis • Low serum bicarbonate, low p. H • Urinalysis – Confirms presence of proteinuria, erythrocyte casts
Glomerulonephritis—Treatment • • Sodium restriction Glucocorticoids Antibiotics Recovery w/ minimal damage – Imp to prevent further exposure to streptococcal infection and recurrent inflam – Adults more difficult • Acute renal failure in 2% • Chronic glomerulonephritis in 10% – Gradually destroys kidneys • Postrecovery testing should be done
Urinary Tract Obstructions: Urolithiasis • Also called: – Calculi – Kidney stones • Frequently reoccur if not treated
Calculi—Pathophysiology • Can develop anywhere in UT; lg or small • Once any solid material or debris forms • Tend to form when: – excessive amts of relatively insoluble salts are in filtrate – Insufficient fluid intake creates highly concentrated filtrate • 75% composed of calcium salts – Remainder: uric acid, struvite, oxalate • Usually cause manifestations only when obstruct flow of urine – Infection if stasis of urine
Kidney Stones
Calculi—Signs and Symptoms • Stones in kidney/bladder frequently asymptomatic • Obstruction of ureter causes attack – “renal colic” • Consists of intense spasms in back and groin • Pain caused by vigorous contractions of ureter – Effort to pass the stone
Calculi—Treatment • Small stones eventually passed out • Larger stones – Extracorporeal shock-wave lithotripsy (ESWL) • Decreases need for invasive surgery – Some drugs can partially dissolve • Need to prevent recurrences
Urinary Tract Obstructions: Tumors —Renal Cell Carcinoma • Primary, silent tumor • Arises from tubule epithelium • Asymptomatic in early stage – Often metastize to liver, lungs, bones, CNS at time of diagnosis • Common after 50 – More freq in males and smokers • Initial sign is painless hematuria • Other manifestations – Dull aching flank pain, palpable mass, anemia • Treatment is kidney removal – 5 yr survival rate 50%