TEVAR Dissections and Aneurysms Christian Shults MD Assistant




 Nicardipine")




















- Slides: 56
TEVAR: Dissections and Aneurysms Christian Shults, MD Assistant Professor, Georgetown School of Medicine Co-Director, Aortic Surgery Director Surgical Ablation Medstar Heart and Vascular Institute
Christian Shults, MD I have no relevant financial relationships
Acute Type B Aortic Dissection • Incidence: 2. 6 -3. 5 per 100, 000 patient-year • Uncomplicated • Complicated – – Malperfusion Rupture Unremitting Pain Uncontrolled HTN
Classic Paradigm Uncomplicated Medical Therapy Complicated Intervention Type B
Uncomplicated – Medical Treatment • • • Labetalol Drip (SBP <120 mm. Hg) Nicardipine Drip Pain Control Serial Exams Labs (Creatinine, Base Deficit, Lactate) Follow up imaging (CTA @ Prior to Discharge, 1, 3, 6, 12 months)
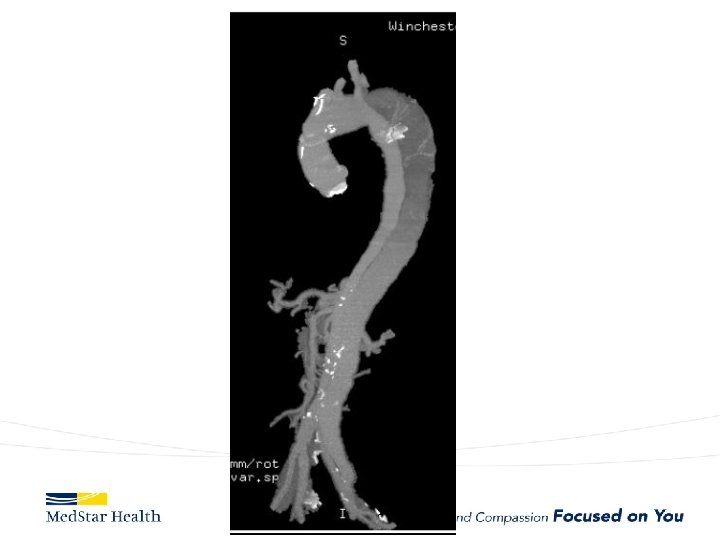
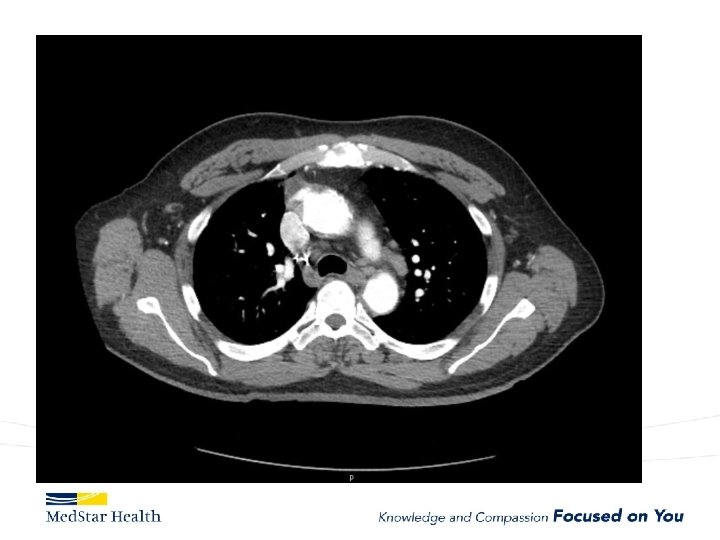
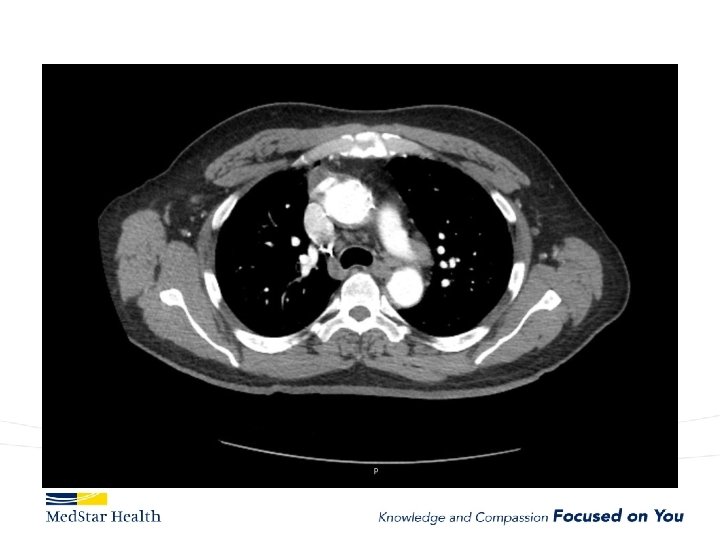
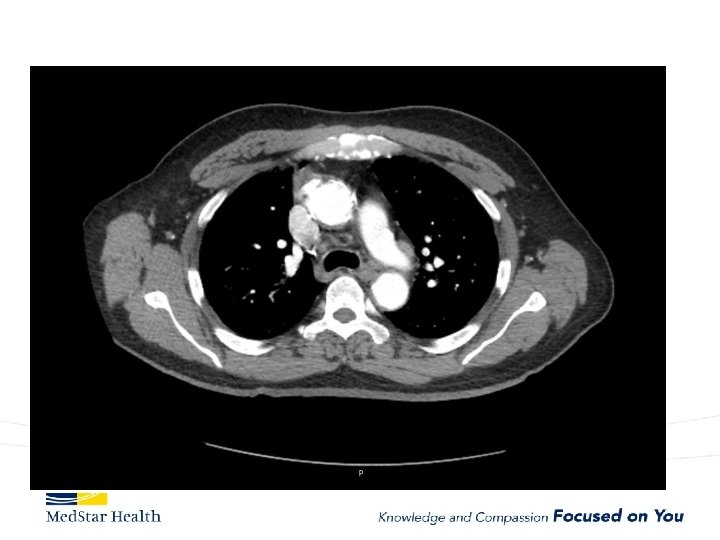
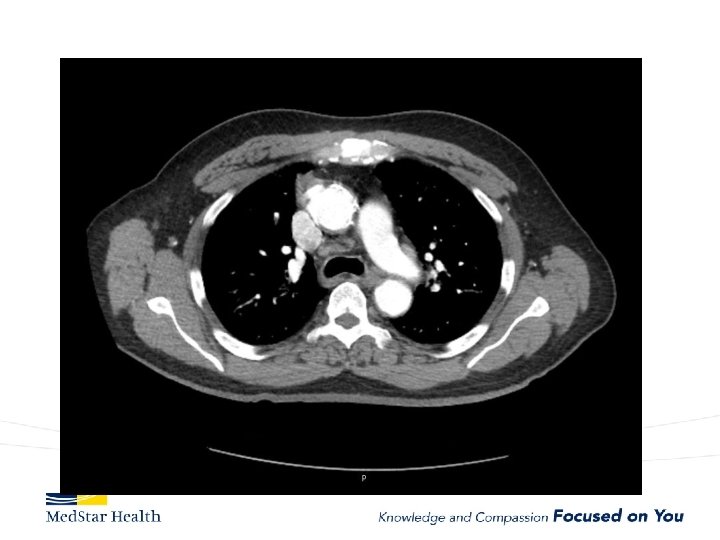
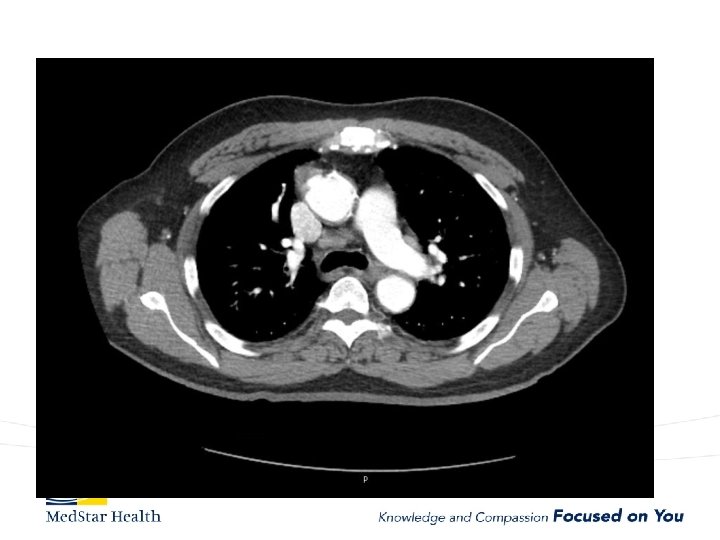
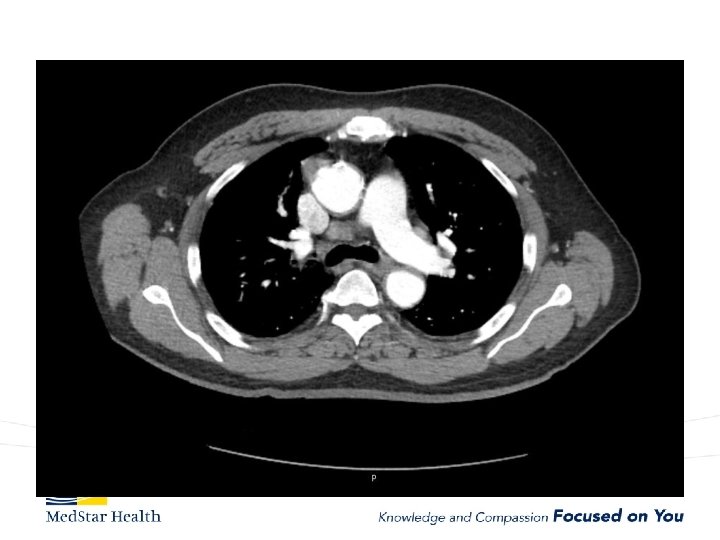
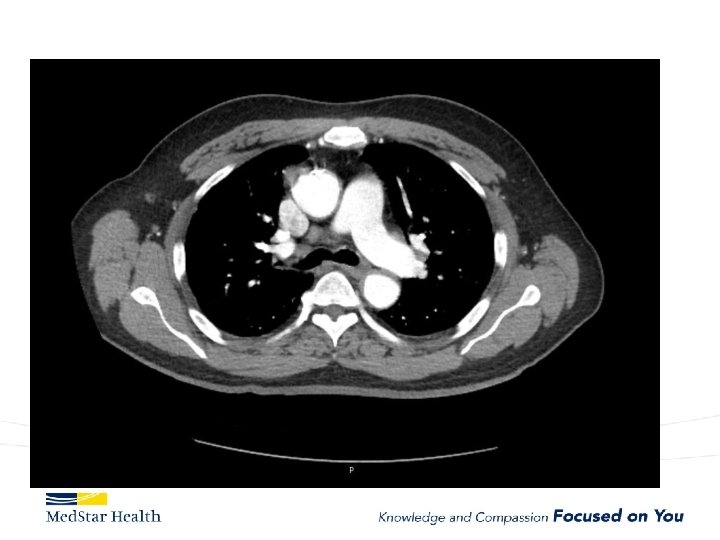
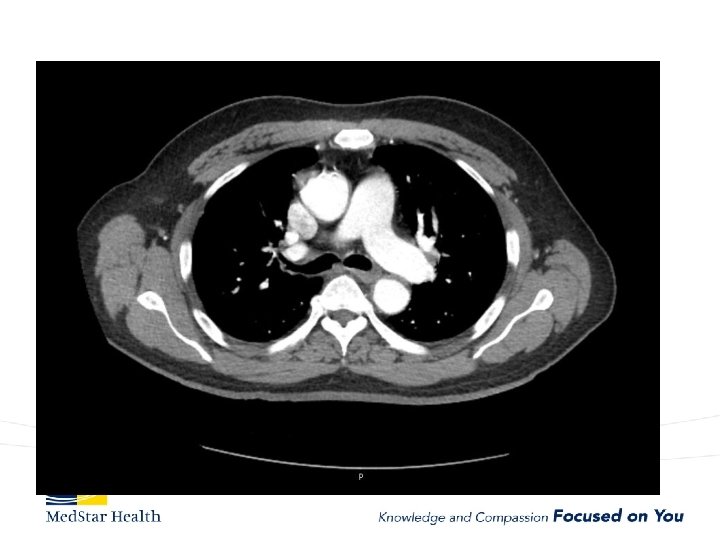
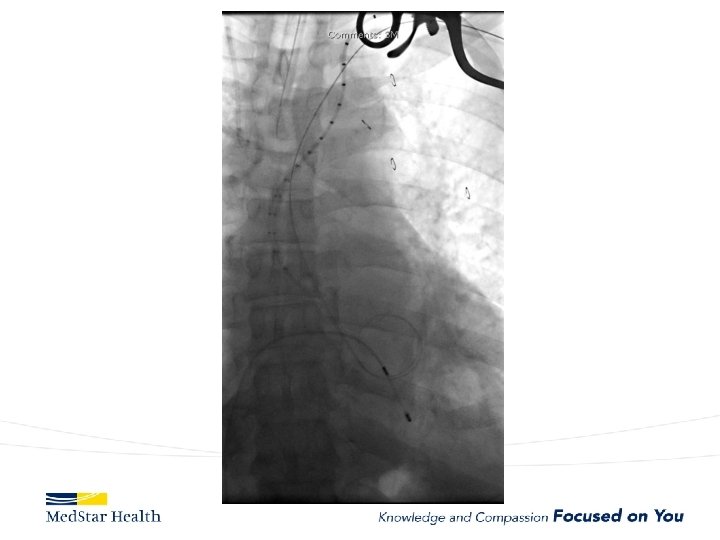
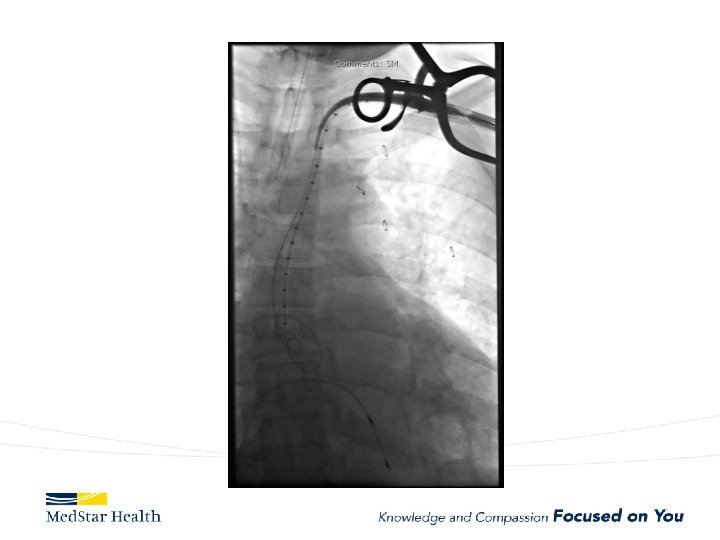
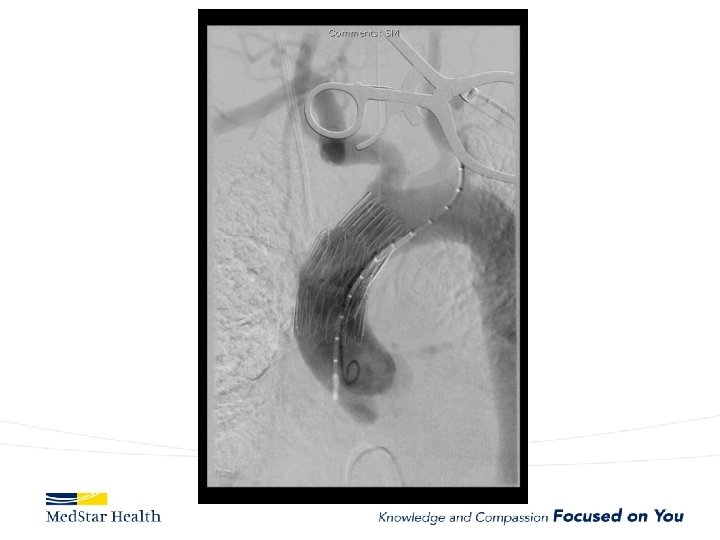
“Uncomplicated” – Type B
Evolving Paradigm – Intervention? • Advantages – Cover primary tear – Aortic Remodeling – Prevent aneurysmal enlargement – Prevent future morbidity/mortality • Disadvantages – – Death SCI Stroke Other complications • MI • Renal failure • Access…
FL
Do We Treat? Who Do We Treat? How Do We Treat?
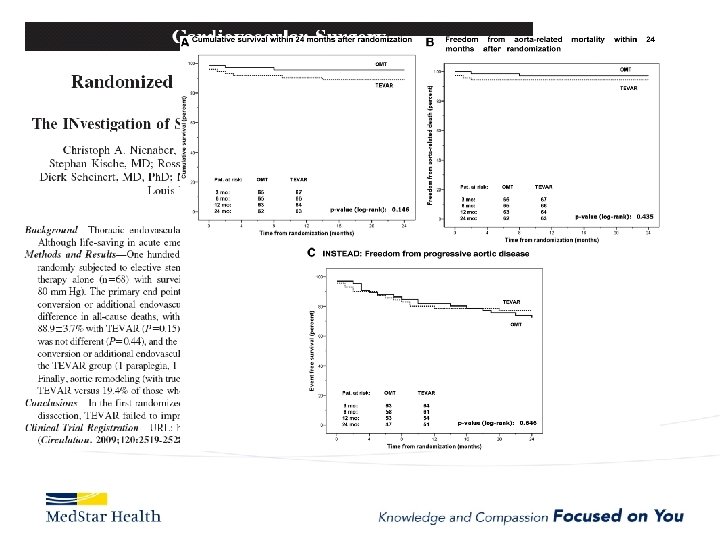
TEVAR demonstrating favorable mortality after 3 yrs INSTEAD trial-Nienaber Veith Symposium 2011
Clinical Evidence INSTEAD XL: Key Results Cumulative Clinical Results: Year 0 through Year 5 19. 1% 46. 1% 12. 4% 27. 0% 19. 3% 11. 1% 6. 9%
IRAD • • 1996 – 2005 390 medical, 59 open surgery, 66 TEVAR In hospital mortality 10. 6% TEVAR, 33. 6% surgery Follow up analysis 1996 -2012 – 276 TEVAR, 5 year mortality 15. 5% – 853 Medical, 29% – TEVAR patients had a higher risk profile (organ ischemia, circulatory compromise, renal failure)
Who Do We Treat?
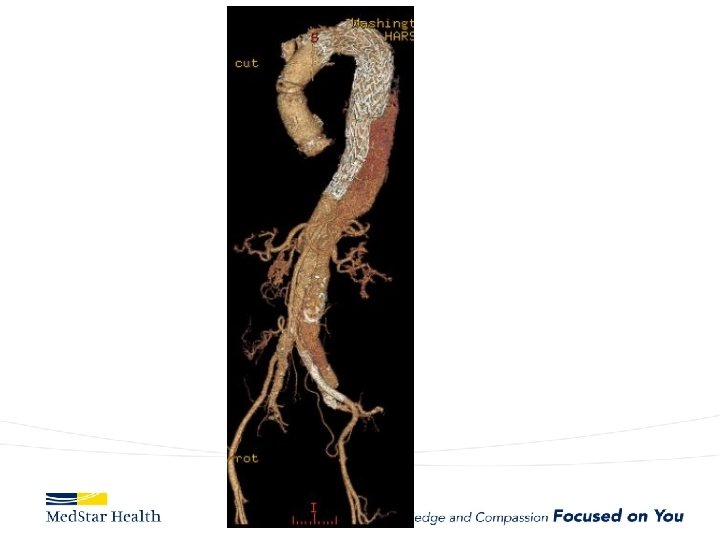
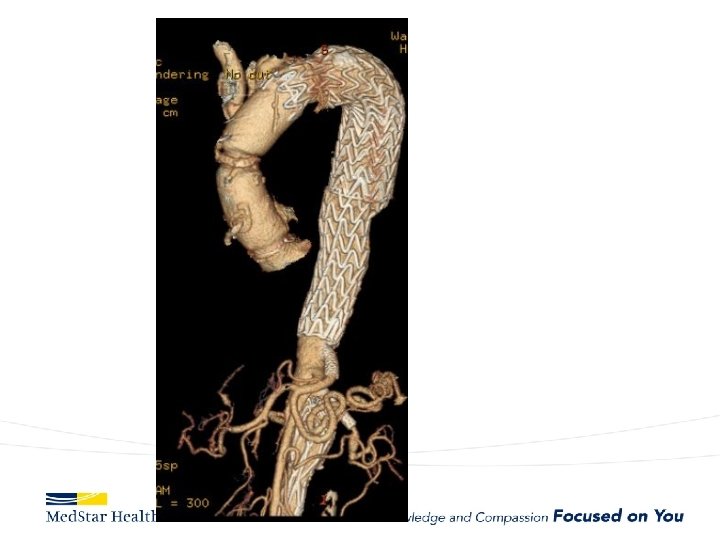
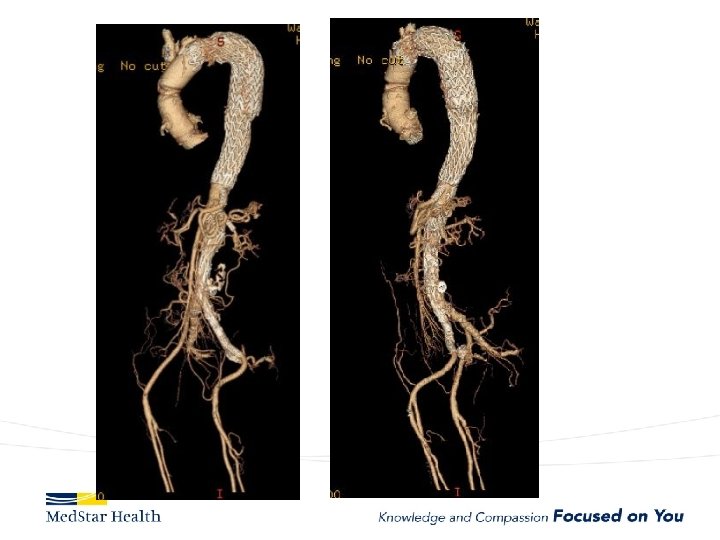
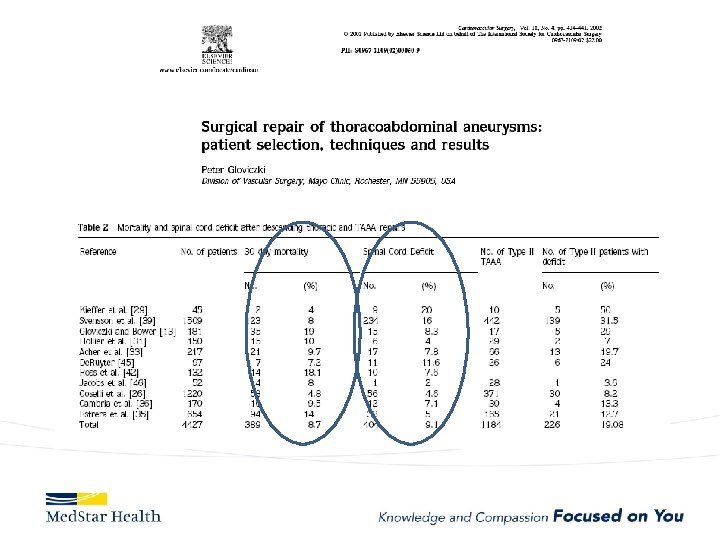
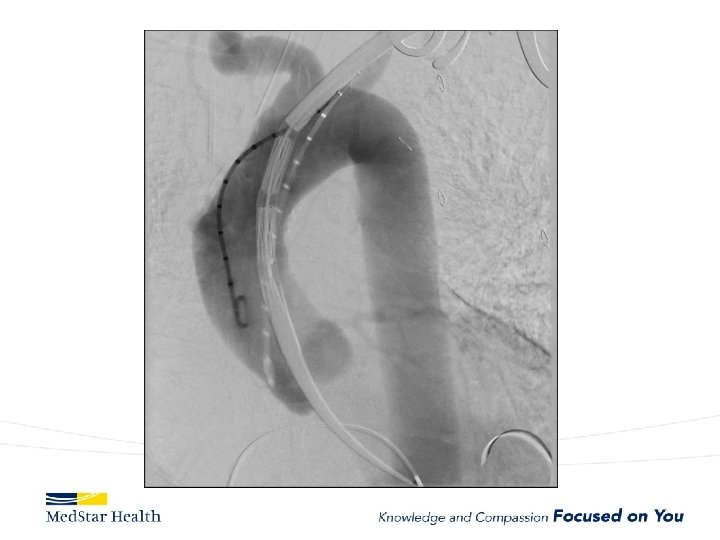
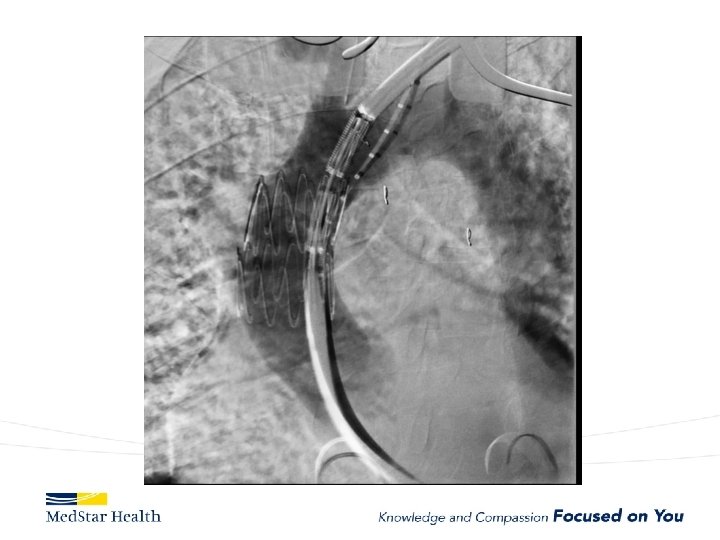
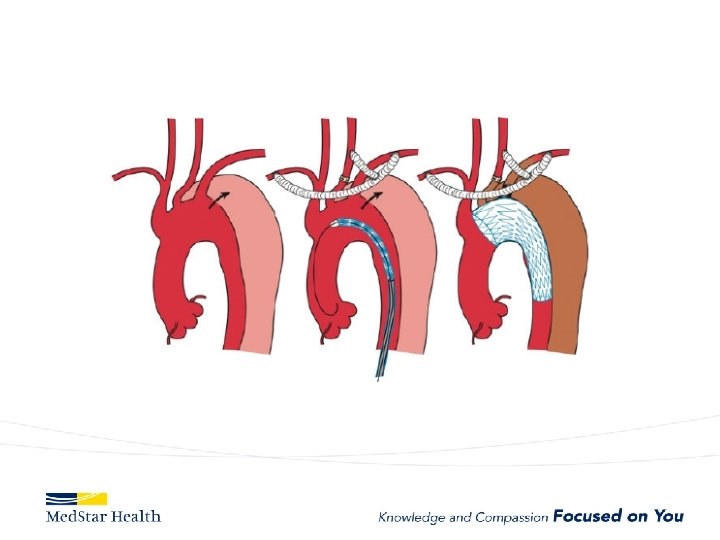
How Do We Treat • Open repair-unacceptable morbidity and mortality • TEVAR – Improved morbidity and mortality – Coverage of primary entry tear – Additional coverage?
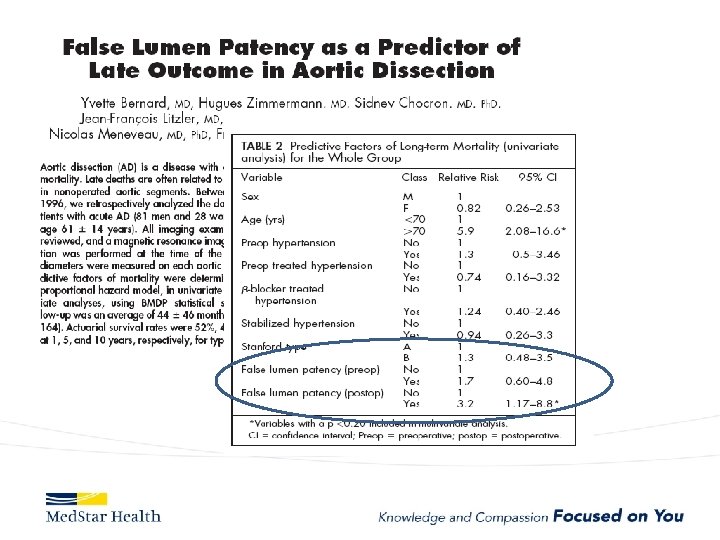
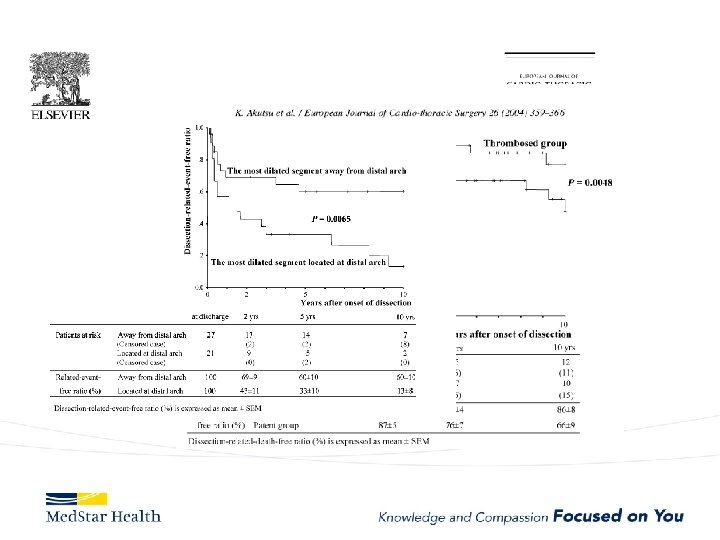
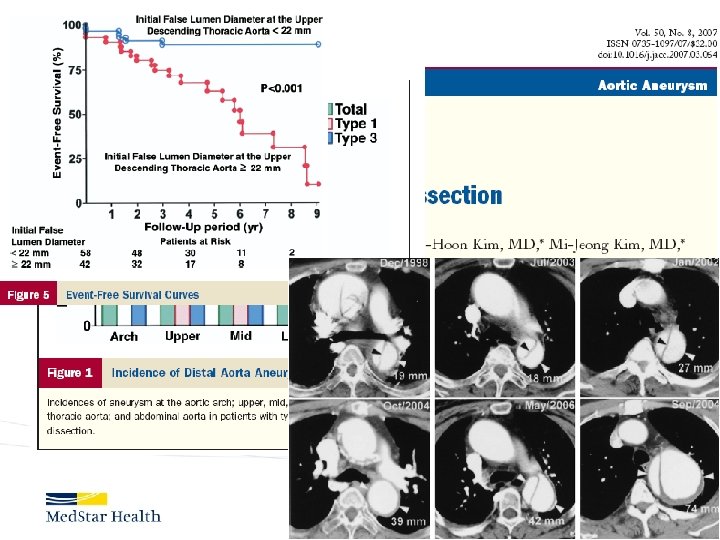
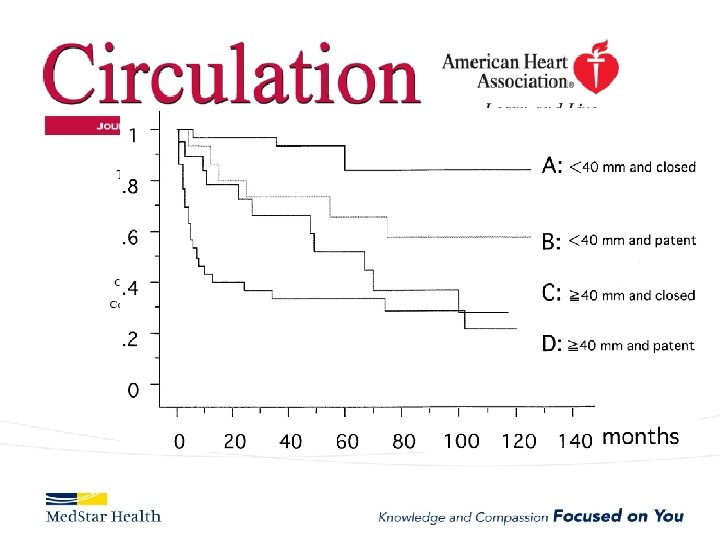
Type B Dissection Complicated Uncomplicated Risk TEVAR age, comorbidities Extreme Low Medical Management False Lumen Small, Thrombosed Medical Management Patent/Large(>22 mm), Total Aorta >40 mm TEVAR/adjuncts
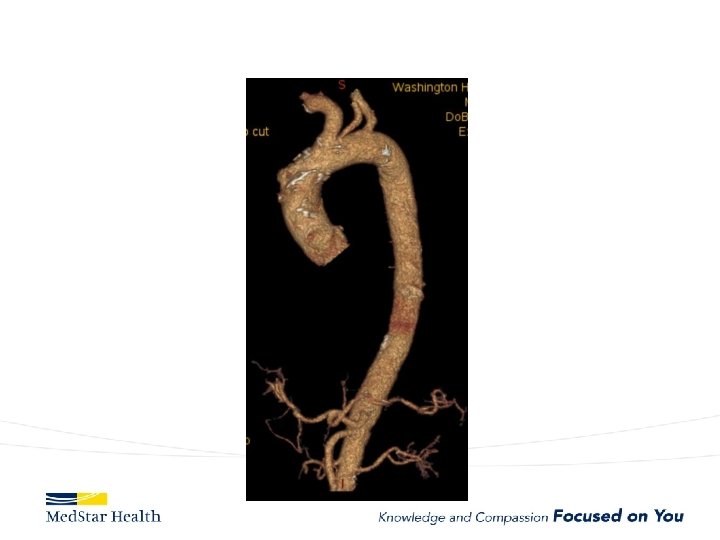
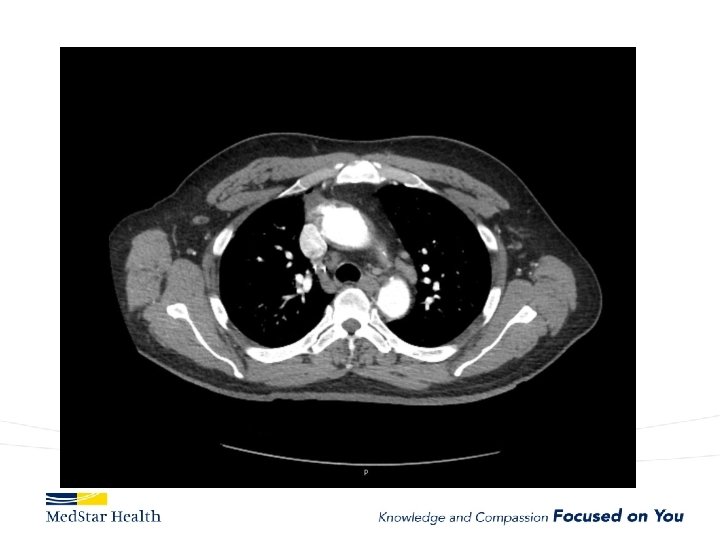
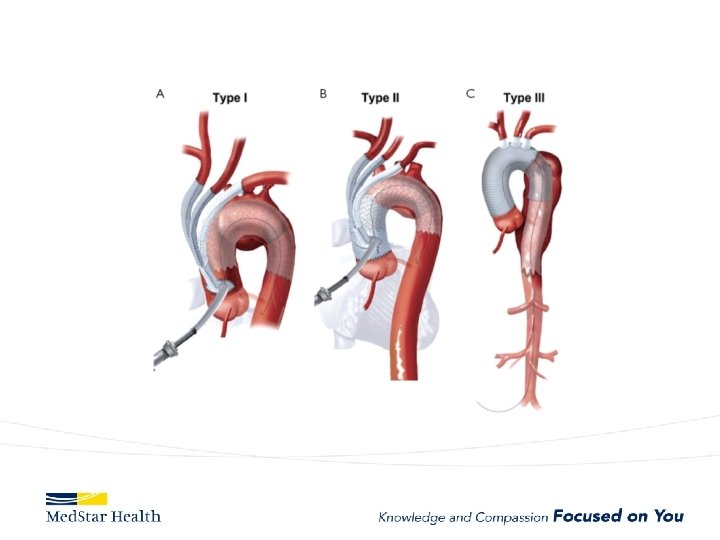
Aneurysms • Descending – Obvious first choice assuming anatomically favorable • Ascending – IDE, Off label in high risk patient • Arch – Available in Europe, Under Trial in US • Thoraco – Available in Europe, Under Trial in US
Ascending Aorta • Currently off label unless in IDE • Challenges – Devices too long or too small for ascending – More complex terrain • Entire cardiac output • Valve/coronaries below • Inomminate above. – New Commercial Devices now available (shorter/tapered)
Current experience with ascending TEVAR JTCVS 2017 Nov 22, Roselli et al. 2006 to 2016 39 patients very high risk for open surgery – A dissection (12, 31%), – intramural hematoma (2, 5%), – pseudoaneurysm (22, 56%), – chronic dissection suture line entry tear (3, 8%). TEVAR in 36 Operative mortality 13%; 5 deaths all in Type A dissections Other complications: – stroke in 4 patients (10%), myocardial infarction in 2 patients (5%), tracheostomy in 2 patients (5%), and dialysis in 2 patients (5%).
• 30 days, 1 year, and 5 years overall survival: – 81%, 74%, and 64% • Freedom from reintervention: – 85%, 77%, and 68% • Significantly higher hazard of mortality with; – zone 0 A versus 0 C (P =. 020) – older age (P =. 026)
Type A Dissection
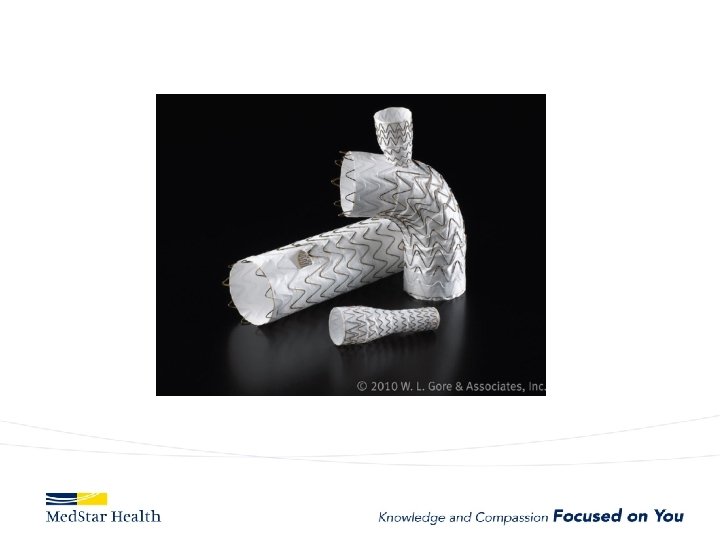
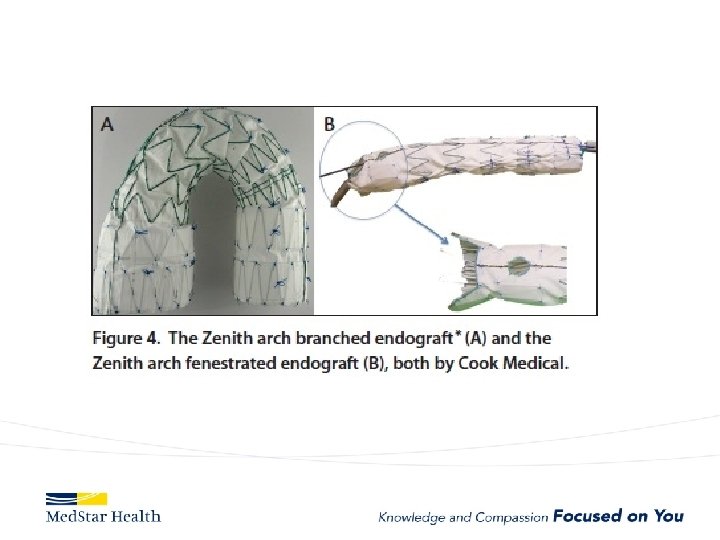
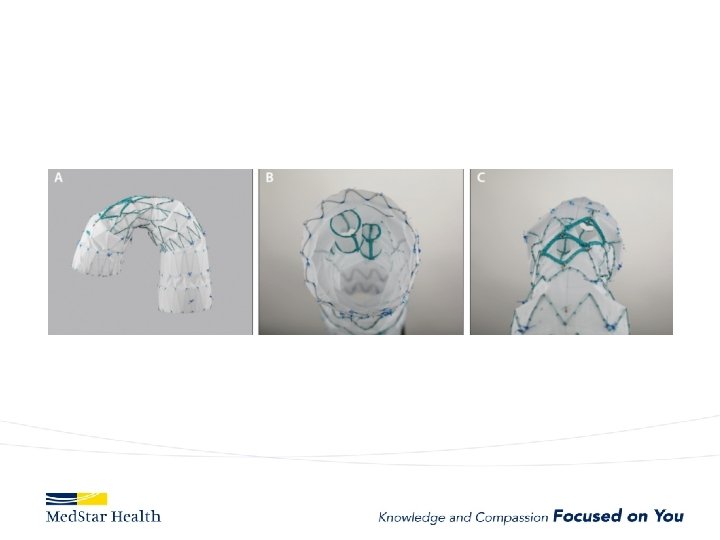
ARCH
Medtronic Mona Lisa
Bolton
Thoraco
Conclusion • Indications for endovascular treatment of aortic disease are evolving • Devices are evolving as well • Future treatment will largely be endovascular