Shock Emergency Approach Part II Cardiogenic shock etiology










ischemia, local")
 • Hypotension with warm and dry")


 CT available immediate * no yes Echocardiography R")
- Slides: 17
Shock - Emergency Approach. Part II
Cardiogenic shock - etiology • Contractility: • AMI • Aneurysm LV • Cardiomiopathy • Myocardium contusion • Acute myocarditis • LV dysfunction (toxics, drugs) • Arrhythmia/ AVB
Cardiogenic shock - etiology • Mechanic problems: – Post partum – – – Acute mitral regurgitation capillary muscles break/dysfunction ASo HCM Aorta dissection Ventricular septum break – – – – Mitral stenosis Atria mixom Massive pulmonary embolism Ventricular septum break Heart break with tamponade Aorta dissection with pericardia tamponade Pericardia tomponade – Pre partum
Pathophysiology- Shock in AMI
Physiopathology • AMI classes- Forrester: – I- CO normal + preload normal ( reperfusion treatment)- mortality 3 % - II- CO normal + pulmonary edema (vasodilatations, diuretic)- mortality 9 % – III- low CO, normal preload (volume, inotrop positive)- mortality 23 % – IV- low CO, preload high ( inotrop positive, vasodilatation) - mortality > 50 %
Clinic framework • Cardiac disease signs: angina pain, dispnea, asthenia • Shock signs • Signs of acute left ventricular insufficiency and right acute ventricular insufficiency
• Anxiety, restlessness, altered mental state due to decreased • • cerebral perfusion and subsequent hypoxia. Hypotension due to decrease in cardiac output. A rapid, weak, thready pulse due to decreased circulation combined with tachycardia. Cool, clammy, and mottled skin (cutis marmorata), due to vasoconstriction and subsequent hypoperfusion of the skin. Distended jugular veins due to increased jugular venous pressure. Oliguria (low urine output) due to insufficient renal perfusion if condition persists. Rapid and deep respirations (hyperventilation) due to sympathetic nervous system stimulation and acidosis. Fatigue due to hyperventilation and hypoxia. Pulmonary edema, involving fluid back-up in the lungs due to insufficient pumping of the heart.
Diagnosis • Physical exam • Ecg 12 leads • Thoracic radiography – pulmonary overloading, ICT • Arterial gases • Myocardium enzymes • Transthoracic and trans esophageal echocardiography • Hemodynamic invasive monitoring
Treatament • Cardiac diseases: trombolysis, PTCA, cardiovascular surgery • APE: mechanic ventilation, vasodilatators, diuretic • Positive inotropic support: dopamine, dobutamine, aortic contra pulsation balloon • Emergency surgeries
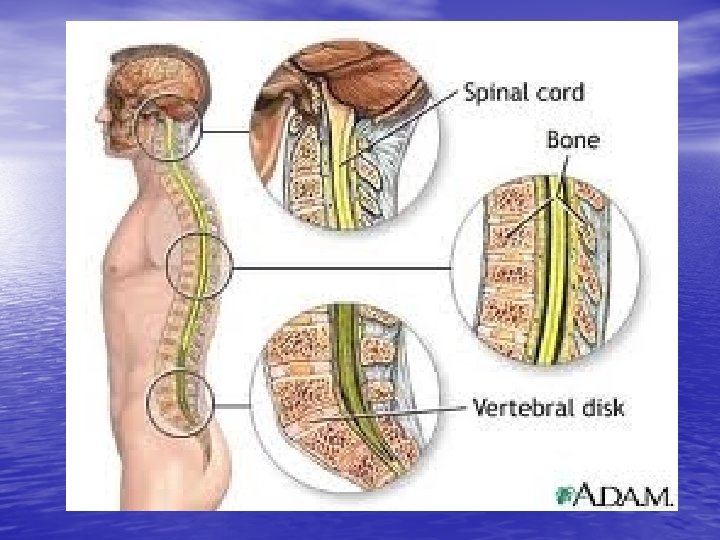
Neurogenic shock - definition • Hypotension and bradycardia appeared after acute lesion of the spine with sympathic influx interruption • Spinal shock – temporary loss of medullar reflex activity appeared after a total spine lesion • Epidemiology – close traumas (car, motobike accidents), open traumas (white weapons, fire weapons)
Physiopathology • Traumatic event: spine compression, dilaceration • Medullar secondary lesions (days, weeks)ischemia, local arterial lesions, intraarterial thromboses • Sympathic tonus loss with emphasis on the parasympathic one • Hypotension, bradycardia
Clinic framework • Traumatic context (close or open) • Hypotension with warm and dry teguments, • • possibly hypothermia Bradycardia Lesion upper than T 1 - blocking of whole SNVS Lesion T 1 -L 3 – partial interruption of SNVS Different framework in penetrative trauma (hemorrhagic component)
Treatament • A- with cervical spine protection • B- ventilation, oxygenation • C- fluids resuscitation: crystalline solutions • D- neurological evaluation • E- secondary evaluation of a patient with trauma • Corticotherapy metilprednisolon 30 mg/kg during • the first hour then 5, 4 mg/ kg/h , 23 h Vasopressor support - dopamine, dobutamine
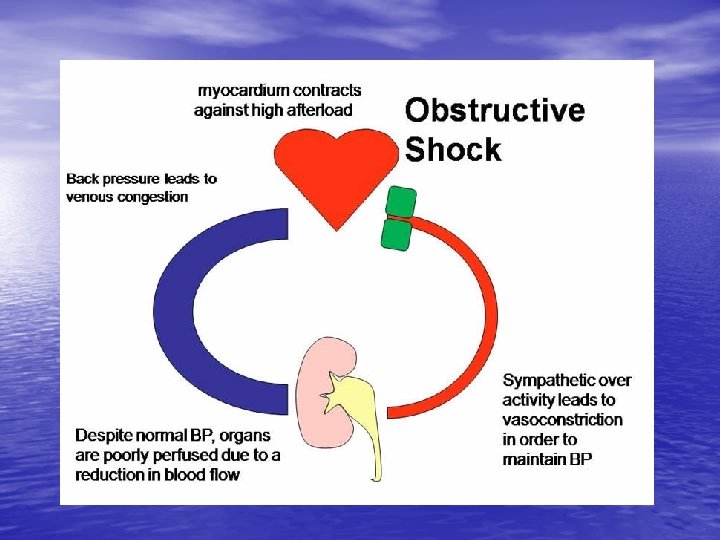
Obstructive shock • Cardiac tamponade • Tension pneumotorax • Massive Pulmonary Embolism • How to recognize? • How to treat?
high risc PE (shock or hypotension) CT available immediate * no yes Echocardiography R V distension no yes CT no availble* alte teste sau pacient instabil Cercetarea altor cauze Tromboliza/ embolectomia nejustificate CT available CT pozitiv Tratamentul specific al EP este justificat Tromboliza sau embolectomi negativ Cercetarea altor cauze Tromboliza/ embolectomia nejustificate