Scapular Dyskinesis Ian S Rice MD Muscles of

 Biceps (long head) Serratus")
















 Definition: Degree loss of internal rotation Measured with shoulder")




















 will respond")
")








- Slides: 52
Scapular Dyskinesis • Ian S Rice MD
Muscles of the Scapula Pec Minor Coracobrachialis Biceps (short head) Biceps (long head) Serratus Anterior Triceps (long head) Subscapularis Rhomboid Major/Minor Levator Scapulae Trapezius Deltoid Supraspinatus Infraspinatus Teres Major Teres Minor Latissimus Dorsi Omohyoid
Infraspinatus Max cross sectional area 1. 8 to 9 times larger compared to supraspinatus and teres minor High eccentric loading during overhead pitching Shortens and limits glenohumeral internal rotation and horizontal adduction ROM Associated with tightness of posterior shoulder structures
Infraspinatus Function Produce glenohumeral joint compression Create a downward pull on the humeral head to minimize superior migration Decelerator during overhead throwing motion Resists shoulder internal rotation and horizontal adduction
Pec Minor Short and tight Increased scapular internal rotation and anterior tilting
Scapula Winging Lateral Winging Medial Winging
Medial Winging Deficit of Serratus Anterior Innervated by long thoracic nerve Caused by repetitive stretch, compression, scapula fx, laceration of nerve Inferior border of scapula goes medial Treatment: Nonop - observe for 6 months for return of nerve function Operative - pec major transfer with fascia lata graft
Lateral Winging Deficit of trapezius Spinal accessory or Dorsal scapular nerve Iatrogenic - ex. dissection for lymph nodes Inferior border of the scapula goes lateral Treatment Eden-Lange transfer Lateralize insertion of levator scapulae and rhomboids
Stages of Throwing
Wind Up Minimal force through the shoulder Inactive rotator cuff muscles Development of torso and leg force
Early Cocking Peak Deltoid activation
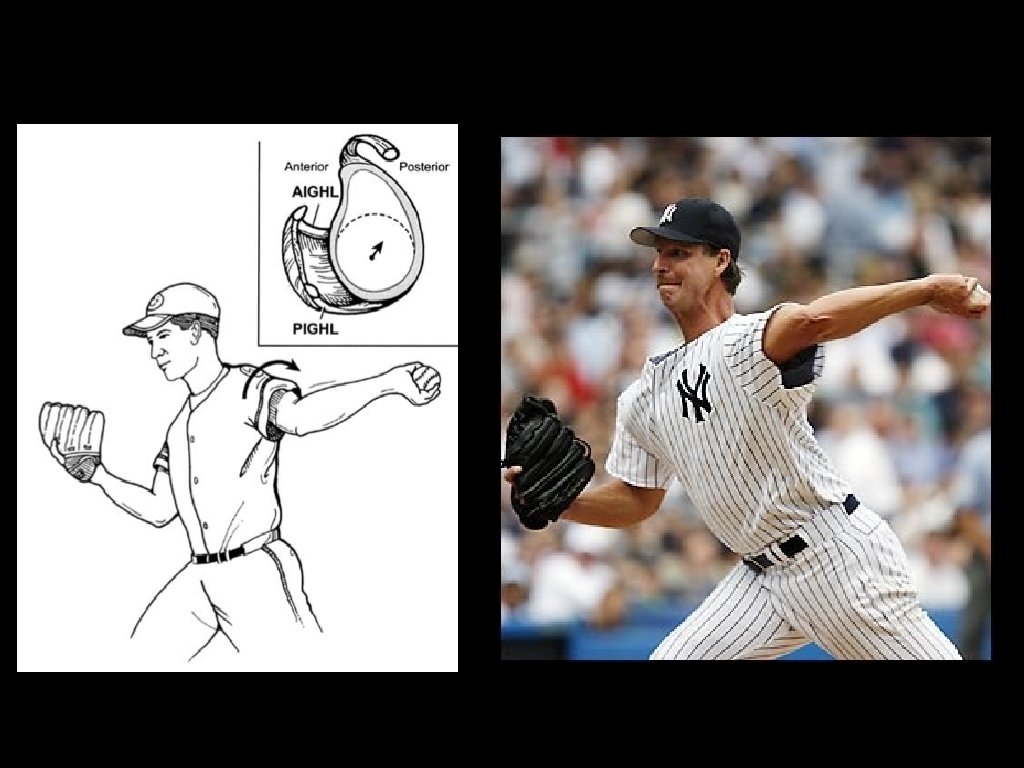
Late Cocking Peak muscle activation: Supra/infraspinatus, teres minor High torque phase: max external rotation of shoulder Glenohumeral internal rotation deficit Internal impingement
Acceleration Triceps activation Pec major, lat dorsi, serratus anterior activation At ball release - 4 body motions Trunk rotation, shoulder internal rotation, elbow extension, wrist flexion 20% reduction in trunk kinetic energy requires 33% more velocity or 70% more mass at distal segments to maintain same energy at ball impact
Deceleration Eccentric contraction of all muscles to counter torque and slow arm motion
Follow Through Distraction forces must be resisted by posteroinferior capsule
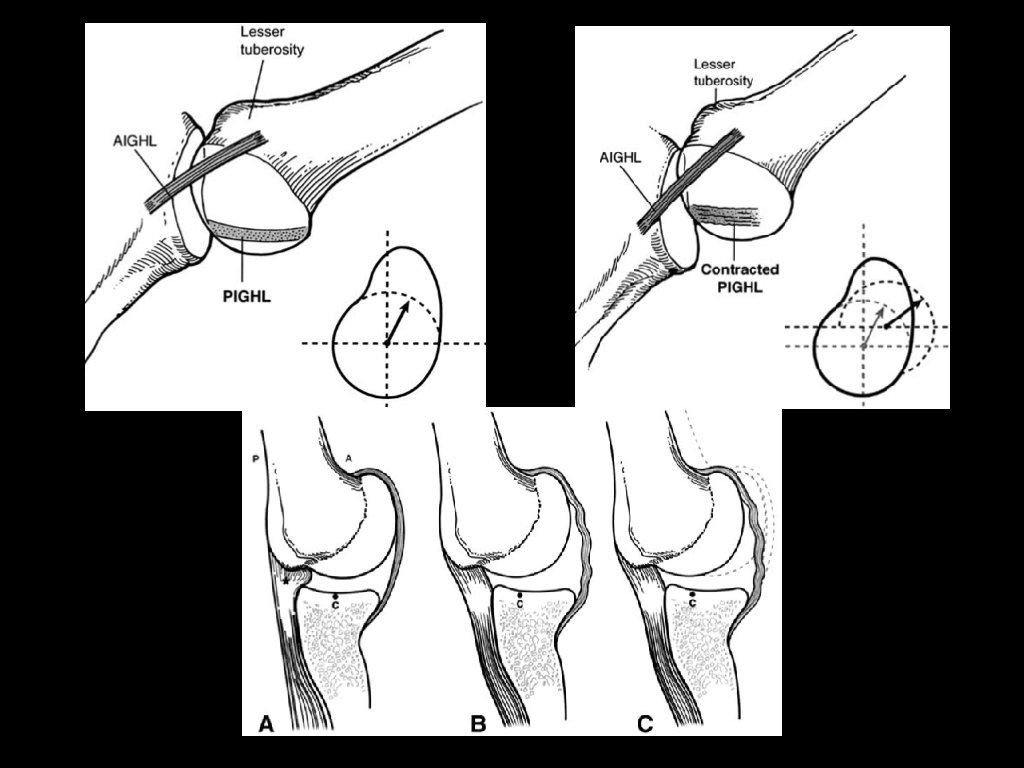
Development of “Dead Arm” Overhead athlete first develops tightness in back of the shoulder Posteroinferior capsular contracture Causes a posterosuperior shift in glenohumeral rotation point Peel back forces in late cocking causes a SLAP lesion Mechanical symptoms dictate surgical treatment Hyperexternal rotation of the humerus increases the clearance of the greater tuberosity over the glenoid and reduces the humeral head cam effect on anterior capsule Scapular protraction develops
Pathoanatomy of “Dead Arm” External rotation forces causes repetitive “microtrauma” to the anterior capsule Hyperexternal rotation and hyperhorizontal abduction Loss of internal rotation in abduction Less than the external rotation gain Caused by posterior inferior capsular contracture Impingement itself is not pathologic All shoulders with in abduction with external rotation show impingement
Glenohumeral internal rotation deficit (GIRD) Definition: Degree loss of internal rotation Measured with shoulder abducted in plane of the body and scapula stabilized by downward pressure to the anterior shoulder Measure to the point where the scapula moves on the posterior chest wall
Tethered Shoulder Posterior capsule contraction Posterior band of the IGHL exerts a posterosuperior force on the humeral head Glenohumeral contact point is shifted and can have more external rotation before impingement Cam effect of the humeral head and proximal humeral calcar on the anteroinferior capsule is reduced by the shift
Development of a SLAP Tear Tight posteroinferior capsule and GIRD develop increased peelback forces and increased shear forces on the labrum Peel back occurs due to bicep tendon vector shifting to a more posterior position in late cocking. Torsional force to rotate medially over corner of glenoid
Role of the Scapula Link between trunk and arm Transfers and increases the energy, power, and equilibrium from lower extremities and trunk Kinetic Chain Theory
Kinetic Chain Coordinated sequencing of multiple segments to maximize power Legs and trunk act as force generators Shoulder acts a funnel and force generator Arm acts as a force delivery mechanism Only 50% of velocity is developed from the arm/shoulder
Kinetic Chain: Legs and Trunk Provides rotational momentum force generation Able to generate 50 -55% of total force and kinetic energy in a tennis serve Weakness in hip abductors or trunk flexors increases lumbar lordosis during arm acceleration Hyperabduction/external rotation position at the shoulder and increases posterior compression loads
Kinetic Chain: Scapula Retracts and protracts around the thoracic wall during the throwing motion Moves with humerus to avoid hyperangulation of humerus on glenoid
The Cascade Acquired posteroinferior capsule contracture Max shear stress on posterosuperior labrum Inferior axillary pouch structures are imbalanced Posterosuperior shift of humeral head Shear forces at biceps anchor and posterosuperior labral attachment increase Anterior capsule structures become lax Excessive external rotation caused by GIRD leads to increased shear and torsional stress in the posterosuperior rotator cuff
Causes of Dyskinesis Bony causes Thoracic kyphosis Clavicle fracture non-union or shortened malunion Joint causes AC instability or arthrosis GH joint internal derangement Neurological causes Cervical radiculopathy Long thoracic or spinal accessory nerve palsy Soft Tissue causes Stiffness of pec minor or short head of biceps —> anterior tilt and protraction GIRD —> reduced humeral head internal rotation and horizontal abduction
Identifying “shoulder at risk” Shoulders with: Glenohumeral internal rotation deficit Malpositioned SICK scapula Anatomy Posterosuperior labrum Posterior supraspinatus tendon Anterior inferior capsular structures
Clinical Clues Medial and inferior scapular borders for winging or prominence Lack of smooth coordinated movement as exemplified by early scapular elevation Shrugging during ascending arm forward flexion and rapid downward rotation during arm lowering from full flexion
Scapular Assistance Test Assisting scapular upward rotation by manually stabilizing upper medial border and rotating the inferomedial border as arm is abducted Positive result Relief of impingement symptoms and weakness
Scapular Retraction Test Manually positioning and stabilizing the entire medial border of the scapula Positive Increased muscle strength Decreased pain with Jobe relocation test
SICK Scapular malposition Inferior medial border prominence Coracoid pain and malposition dys. Kinesis of the scapular movement Clinical Presentation Anterior shoulder pain (coracoid) , posterosuperior scapular pain, superior shoulder pain, proximal lateral arm pain Inferior position, lateral displacement, abduction
SICK Scapula Coracoid pain with passive forward flexion Pec minor & short biceps tendon “tightness” Lowers leading edge of acromion causing impingement from anteroinferior angulation Levator scapulae is placed under tension when scapula tilts and rotates laterally Decreased subacromial space
Patterns of Dyskinesis Type I - inferior medial scapular border prominence Type II - medial scapular border prominence Type III - superomedial scapular border prominence
Poor posture Prolonged sitting tasks leads to forward head posture, increased thoracic kyphosis, and protraction of shoulder girdle Reduced clavicle retraction Increased clavicle elevation Scapular upward rotation Scapular posterior tilt Slouched posture affects scapular orientation, shoulder muscle strength and ROM Altered serratus anterior muscle activity Force imbalance in upper and lower trapezius muscle Flexibility deficits (pec minor tightness, posterior glenohumeral capsular stiffness)
Dyskinesis and Neck Pain No consensus about relationship Noted to be a risk factor for shoulder pain Possible predisposition to develop shoulder pain, and then is exacerbated by it Typical finding of bilateral scapular dyskinesis in patients with shoulder pain Worse on affected side
Rehabilitation Need to determine patient goals Office worker: correction of axioscapular muscles, scapular orientation with arms by the sides, and during prolonged upper limb activities Overhead Athletes: advanced scapular muscle control and strength in sport specific movements
Need to address whether flexibility deficits are primary or secondary If flexibility is the issue, then address that prior to motor control learning
Rehab of Flexibility Defects Scapular level Pec Minor and Levator Scapulae Scapular retraction in 30 deg of flexion Largest change in pec minor length Glenohumeral Level Posterior shoulder structures, capsule, external rotator muscles Sleeper stretch
Sleeper Stretch 90% of throwers with symptomatic GIRD (greater than 25 deg) will respond to stretching. Acceptable: less than 20 deg or less than 10% of total rotation in non throwing shoulder. Period of time: 2 weeks
Rehab of Muscle Motor Control Neuromuscular deficits (lack of cocontraction and force couple activity) Upper Trap hyperactivity Strength deficits Serratus anterior, Middle and Lower Trap
Conscious Muscle Control Activating Lower Trap Patient palpates coracoid and then focuses on “pulling the coracoid from his finger and moving the scapula backwards” Creates posterior tilt and upward rotation Counters a SICK scapula Spinal Posture Correction Neutral lumbopelvic posture, with correction of scapulothoracic and cervical postures “Occipital lift” of the head
Muscle Control and Strength Open Chain Exercises Low Row, Inferior Glide, Lawnmower Closed Chain Exercises - require less activation than open chain Pushing hands on thighs in upright sitting, Wall sliding exercise, Pushups Want exercises with low Upper Trap/Lower Trap, Upper Trap/Middle Trap, and Upper Trap to Serratus Anterior ratios Support the arm (wall slide and bench slide exercises) Intramuscular Trapezius training Side lying external rotation, side lying forward flexion, prone horizontal abduction with external rotation and prone extension Early activation of lower trapezius Diagonal patterns including lower limb and core muscle activity favor scapular muscle activity (lower trapezius)
Low Row Trunk extension, scapular retraction, arm extension as patient pushes posteriorly
Wall Washes
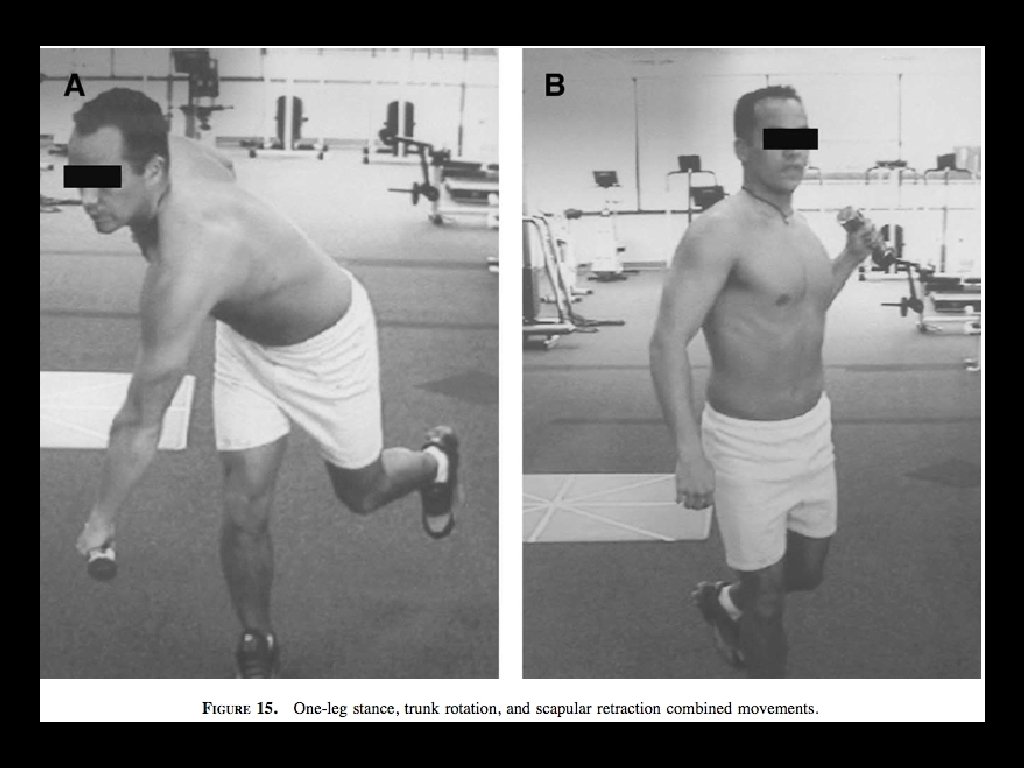
Advanced Sports Movements Last stage of rehab Goal: exercise advanced scapular muscle control and strength Attention to integration of the kinetic chain into the exercise program, plyometric and eccentric exercises Throwers use weight balls and elastic resistance tubing Swimmers should focus on exercises while prone W-V exercise Total Time: 12 weeks to 6 months
Summary Posterior inferior capsular contracture Leads to GIRD Then posterior superior cuff internal impingement Which develops posterosuperior SLAP tear Resulting in Anterior capsular stretching Scapular protraction
OITE 23 yo professional pitcher complains of posterior shoulder pain. Physical exam is notable for scapular dyskinesis. No intra-articular pathology is found on shoulder MRI. Which of the following should be emphasized in the initial stages of rehabilitation? 1) Isometric shoulder exercises 2) Isokinetic shoulder exercises 3) Closed chain shoulder exercises 4) Coordination of scapular motion with trunk and hip movements 5) Axial loading shoulder exercises
4 Scapular dyskinesis is an alteration in the normal motion of the scapular during coordinated scapulohumeral movements. It occurs as a sequela of prior shoulder injury, especially injuries disrupting the activation patterns of scapular stabilizing muscles. Kibler et al outlined a rehabilitation protocol to treat scapular dyskinesis. The principle is to treat the problem proximal to distal. The first stage involves attaining full motion of the scapular and coordinating the scapula with trunk and hip motions. Once this has been achieved, the second stage involves strengthening the scapular musculature. As scapular control is attained, exercises are introduced that place emphasis on the shoulder and arm beginning with flexibility and closed-chain strengthening, eventually working up to sport-specific functions. Progress is determined by functional improvement rather than a strict time table.